

Autor :Varas, HÃĐctor1, SÃĄnchez, Ãngel1,Amarilla, YÃĐsica1, GarcÃa, Artemio1, Benavides, Alejandra1, Cabral, Daniela1, Antunovich, Federico2, Caballero, Andrea2, Figueredo, Heber3,Benavente, Emilio3
1Pulmonology Service - High Complexity Hospital - Formosa - Argentina
2Surgery Service - High Complexity Hospital - Formosa - Argentina
3Rheumatology Service - High Complexity Hospital - Formosa â Argentina
https://doi.org/10.56538/ramr.DFVP9823
Correspondencia : HÃĐctor Varas E-mail: hectorvaras94@gmail.com
RESUMEN
La
enfermedad de Fabry pertenece al grupo de enfermedades lisosomales, poco
frecuenÂtes y de origen genético. Se comporta como una enfermedad
crónica, multisistémica y progresiva, que deteriora la calidad de
vida y disminuye la supervivencia del paciente.
La
afectación pulmonar en esta enfermedad es incierta y no existen reportes
en la bibliografía sobre su incidencia. Presentamos el caso de un
paciente masculino con diagnóstico de enfermedad de Fabry y compromiso
pulmonar.
Palabras
claves: Neumotórax
espontáneo; Enfermedad de Fabry; Enfermedad lisosomal
ABSTRACT
Fabry
disease belongs to the group of lysosomal diseases, which are rare and of
genetic origin. It behaves like a chronic, multisystemic, progressive disease
that deteriorates the quality of life and decreases patientâs survival.
Lung
involvement in this disease is uncertain, and there are no reports in the
literature related to its incidence. We present the case of a male patient with
a diagnosis of Fabry disease and lung involvement.
Key
word: Spontaneous
pneumothorax;
Fabry disease; Lysosomal disease
Receved: 08/11/2022
Accepted: 02/24/2022
CASE REPORT
Medical history
22-year-old
male patient, from the city of Formosa, diagnosed with Fabry disease since
2018, and cuÂrrently undergoing enzyme replacement therapy. The patient denies
a history of smoking or use of illicit substances. No other pathological
history reported.
Reason for consultation
The
patient reports having started with dyspnea and chest pain of 8/10 intensity 6
days prior to admission. He claims it was a stabbing type of pain that radiated
throughout the left hemithorax and shoulder. He also stated that the pain
intensity increased when lying on the affected side. And he denies any other
associated respiratory symptoms. He decided to consult his primary care
physician, who requested a chest X-ray.
As
a previous history, the patient reports having had a pain of similar
characteristics the previous year, which resolved spontaneously.
Physical examination
The
patient is eupneic, with a SpO2 of 98% on room air. There is a marked
decrease in the vesiÂcular murmur in the left hemithorax, without any added
sounds. Lower excursion of the homolateral lung base.
Laboratory
tests: complete blood count, liver function test, and renal function test
results are normal.
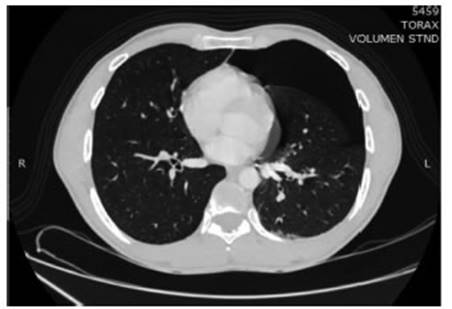
Chest
CAT: left pneumothorax predominantly affecting the anterior and basal regions.
No
consolidative opacities or ground-glass opaÂcities are recognized in assessable
sections of the lung parenchyma.
Supplementary testing
Evolution
Given
the absence of any other triggering cause, the condition is assumed to be a
spontaneous pneumothorax, and the decision is made, together with the thoracic
surgery team, to place a pleural drainage tube.
During
hospitalization, the patient showed good clinical and radiological evolution;
therefore, he was discharged.
DISCUSSION
Fabry
disease is a genetic disorder with X-linked inheritance, caused by a deficiency
in the activity of the lysosomal enzyme alpha-galactosidase A.1-3
In
most cases, it is due to deficiencies in lysoÂsomal hydrolytic enzymes,
although it can also be due to alterations in lysosomal membrane proteins and
those associated with the synthesis of lysosoÂmal proteins. It is characterized
by the deposition of globotriaosylceramide (Gl3 or Gb3) in different organs and
tissues, with frequent involvement of the skin, the digestive system, the
cornea, and more severely, in the nervous system, heart, and kidneys.2

Incidence:
Fabry disease has an approximate incidence of 1 in every 117,000 live births
and 1 in every 40,000 men, and is one of the most common lysosomal storage
disorders. Recently, it has been discovered that its prevalence is higher in
patients undergoing hemodialysis, young patients with cerebrovascular accident
(CVA) or left ventricular hypertrophy (LVH) of unknown origin, compared to the
general population.2
The
diagnosis of this disease is made by demonsÂtrating a decreased enzyme
function, after which a confirmatory genetic study is conducted.3
Lung
involvement in Fabry disease, and its seÂverity, remain a controversial topic,
as there are very few publications on the subject.
In
a systematic review by Svensson et al, the main findings include: intermittent
chest tightness, pneumothorax, hemoptysis, recurrent pulmonary infections,
pulmonary thromboemboÂlism, and pulmonary infarction.4
In a case series published by Brown, 3 patients with spontaneous
pneumothorax in Fabry disease were described: two were associated with bullous
changes in chest radiography and one was associated with pulmoÂnary emphysema
in the autopsy.5
In
the case of our patient, where no probable causes of pneumothorax were
identified and it was assumed to be spontaneous, it is still possiÂble to
consider a potential association with the underlying disease. Due to the
limited number of reports on the pulmonary and pleural presentation of this
disease, it was decided to present this case.
Conflict
of interest
The
authors have no conflict of interest to declare.
REFERENCES
1.
AADELFA (Asociación Argentina de estudio de enfermedad de Fabry y otras
enfermedades lisosomales). Evaluation of patients with Fabry disease in Argentina. Medicina (B Aires). 2010;70:37-43.
2.
Neumann P, Antongiovanni N, Fainboim A, et al. Guía para el
diagnóstico, seguimiento y tratamiento de la Enfermedad de Fabry.
Consenso de médicos de AADELFA Y GADYTEF. Medicina Buenos Aires. 2013;73:482-94.
3.
Gonzalez-Rodriguez J, Benavidez-Villalobos J, Arroyo Villalta A Enfermedad de
Fabry en el adulto: revisión bib-liográfica. RHCS 2020;6:75-84. https://doi.org/10.56239/rhcs.2020.62.430
4.
Svensson CK, Feldt-Rasmussen U, Backer V. Fabry disease respiratory symptoms,
and airway limitation - a systematic review. Eur Clin Respir J. 2015;2.
https://doi.org/10.3402/ecrj.v2.26721
5.
Brown LK, Miller A, Bhuptani A, et al. Pulmonary involvement in Fabry disease.
Am J Respir Crit Care Med. 1997;155:1004-10
https://doi.org/10.1164/ajrc-cm.155.3.9116979

| GalerÃa de imÃĄgenes | ||
| Mujer joven con afectaciÃģn pulmonar bilateral y alteraciÃģn de la conciencia | ||
Autores: Churin Lisandro |
 |
|