

Autor : Falduti, Alejandra1, Catini, MarĂa Eugenia1, Chiappero, Guillermo1
1 Hospital General de Agudos Juan A. Fernández, Autonomous City of Buenos Aires, Argentina
https://doi.org/10.56538/ramr.PTWI9302
Correspondencia : Falduti Alejandra E-mail: alejandrafalduti13@gmail.com
ABSTRACT
Introduction:
Patients
with severe COVID-19 pneumonia may require orotracheal intubation, prolonged
mechanical ventilation, and tracheostomy. The presence of a tracheostomy
cannula does not contribute by itself to the development of dysphagia, but the
frequency of dysphagia in these patients is high and with risk of aspiration.
Objective:
To
describe the prevalence of oropharyngeal dysphagia in patients who required
tracheostomy after prolonged mechanical ventilation secondary to COVID-19,
assessed by an instrumental method. As a secondary objective, to evaluate the
asÂsociation between the presence of dysphagia and clinical-demographic
variables, the duration of invasive mechanical ventilation, days of artificial
airway, presence of laryngeal injuries, and length of stay in the Intensive
Care.
Methods:
Observational,
longitudinal, retrospective study conducted at the Hospital Juan A.
Fernández, Autonomous City of Buenos Aires (CABA), Argentina. TracheosÂtomized
patients diagnosed with COVID-19 were consecutively included in the study. The
presence of dysphagia was assessed by an endoscopic study of swallowing at the
time of decannulation.
Results:
A
total of 69 tracheostomized patients undergoing decannulation were included in
the study. 65 of these patients were evaluated through swallowing endoscopy,
and 50 were diagnosed with dysphagia (76.9 %). The median number of
tracheostomy days was 32. When comparing tracheostomy days between the group
without dysphagia (median of 21 days) and the group with dysphagia (median of
36 days), statistically significant differences were reported between both
groups (p=0.015).
Conclusion:
Oropharyngeal
dysphagia was prevalent in this cohort of COVID-19 paÂtients. A significant
association was found between patients with more tracheostomy days until
decannulation and the development of dysphagia.
Key
words: Covid-19,
Decannulation, Swallowing, Dysphagia, Laryngeal injuries
RESUMEN
Introducción:
Los
pacientes con neumonía grave por COVID-19 pueden requerir inÂtubación
orotraqueal, ventilación mecánica prolongada, y
traqueostomía. La presencia de una cánula de traqueostomía
no implica por sí misma el desarrollo de disfagia, pero la frecuencia de
disfagia en estos pacientes es alta con riesgo de aspiración.
Objetivo:
Describir
la prevalencia disfagia orofaríngea en pacientes que requirieron
traqueostomía luego de ventilación mecánica prolongada
secundaria a COVID-19, valorada mediante un método instrumental. Como
objetivo secundario, evaluar la asociación entre la presencia de
disfagia y variables clínico-demográficas, duración de la
ventilación mecánica invasiva, días de vía
aérea artificial, presencia de lesiones laríngeas y días de
estadía en terapia intensiva.
Métodos:
Estudio
observacional, longitudinal y retrospectivo, realizado en el hospital Juan A.
Fernández, CABA, Argentina. Se incluyeron de manera consecutiva
pacientes con diagnóstico de COVID-19 traqueostomizado. La presencia de
disfagia se valoró mediante estudio endoscópico de la
deglución al momento de la decanulación.
Resultados:
Un
total de 69 pacientes traqueostomizado en proceso de decanulación
ingresaron al estudio. De ellos, 65 pacientes fueron analizados y evaluados
mediante endoscopía de la deglución y 50 se diagnosticaron con
disfagia (76,9 %). La mediana de días de traqueostomía fue de 32;
al comparar los días de traqueostomía entre el grupo sin disfagia
(mediana 21 días) y el grupo con disfagia (mediana 36), se observaron
diferencias estadísticamente significativas entre ambos grupos (p=0,015).
Conclusión:
La
disfagia orofaríngea fue prevalente en esta cohorte de pacientes con
COVID 19. Los pacientes que tuvieron más días de
traqueostomía hasta la decanulación se asociaron
significativamente con el desarrollo de disfagia.
Palabras
claves: Covid19,
Decanulación, Deglución, Disfagia, Lesiones laríngeas
Received: 12/12/2023
Accepted: 03/15/2024
INTRODUCTION
The
tracheostomy (TQT) is one of the most freÂquently performed procedures in the
Intensive Care Unit (ICU), with a prevalence of 10 to 15 % of ventilated
patients in a multipurpose unit.1,2 The most common
indications include prolonged meÂchanical ventilation, facilitating access for
proper bronchial hygiene, and prevention of laryngeal injuries secondary to
orotracheal intubation (OTI), also as treatment for upper airway obstruction.3 As an
advantage, we can say that it facilitates oral feeding, phonation, patient
well-being, and reduces the use of sedatives.4
On
March 11, 2020, the World Health OrganiÂzation (WHO) declared coronavirus
disease 2019 (COVID-19) as a pandemic5; approximately 1 every 5 infected
people required hospitalization, while 1 every 10 could be admitted to the ICU.
Most of these patients required OTI and invasive meÂchanical ventilation (IMV)
due to acute respiratory distress syndrome.6,7
Williams
et al point out that TQT rates during the pandemic range from 16 % to 61 %,
significantÂly higher than before the pandemic. Additionally, according to the
Argentine study SATICOVID, approximately one-quarter of patients on IMV were tracheostomized.8,9
Although
the TQT itself does not imply the development of dysphagia, it occurs in 11 %
to 93 % of tracheostomized patients. The presence of the TQT cannula causes the
cessation of the translaryngeal airflow, leading to laryngeal desenÂsitization,
glottic closure lack of coordination, and disuse atrophy of the swallowing
muscles, which can result in dysphagia.10.11
There
is growing evidence that the chronicity and severity of the underlying disease,
the comorÂbidities, and recent intubation are determining factors of dysphagia
in this patient population; therefore, it should be diagnosed and treated to
prevent severe respiratory complications, severe nutritional compromise, even
death.12
The
decannulation of patients with prolonged TQT is not simple, and particularly
patients with marginal respiratory reserve and dysphagia are at higher risk of
decannulation failure.13
The
primary objective of this study was to deÂscribe the prevalence of
oropharyngeal dysphagia in patients who required TQT following prolonged
mechanical ventilation secondary to COVID-19, assessed through an instrumental
method using a fiberoptic endoscopic evaluation of swallowÂing (FEES). This
study can be performed at the patient’s bedside and allows for the evaluation
of laryngeal and pharyngeal structures, laryngoÂpharyngeal sensitivity, saliva
management, and swallowing of different food consistencies.14
A
secondary objective was to evaluate the asÂsociation between the presence of
dysphagia and clinical-demographic variables, duration of IMV, days with
artificial airway (AA), presence of larynÂgeal injuries, and length of stay in
the ICU.
MATERIALS AND METHODS
This
study was conducted in the ICU of the Hospital GeÂneral de Agudos Dr. Juan A.
Fernández (HGAJAF), in the Autonomous City of Buenos Aires, Argentina,
from May 2020 to December 2021. The study design was observatioÂnal,
retrospective, and cross-sectional.
Patients
older than 18 years admitted to the HGAJAF who had a diagnosis of COVID-19 at
hospital admission were consecutively included. Those patients required meÂchanical
ventilation (MV) and TQT, and once they were weaned off, they were referred by
the treating medical team to begin the decannulation process.
The
following demographic and clinical data were reÂcorded: age, sex, personal
history, and days of OTI, TQT and IMV. Additionally, the length of stay in the
ICU was calculated.
The
blue dye test was performed when the patient was able to breath spontaneously
without ventilatory support for at least 12 hours. This moment was considered
the start of the decannulation process, and the result was recorded as positive
or negative.
At
the time of decannulation, the following elements were evaluated: the presence
of delirium using the CAM-ICU tool (Confusion Assessment Method for the
Intensive Care Unit); the maximal expiratory pressure (Pemax) with a manometer
and through the TQT cannula with the balloon inflated; peak cough flow (PCF)
with occlusion of the TQT cannula and with an oronasal mask; and the peripheral
muscle strength using the Medical Research Council (MRC) scale.
The
fiberoptic endoscopic evaluation of swallowing (FEES) was performed on all
patients at the time of decannulation, according to the technique described by
Langmore.15
The
study was conducted by an intensive care physician and a kinesiologist using a
disposable flexible videoscope (Ambu®
aScope™). Initially, anatomical structures, vocal cord mobility,
and glottic closure were evaluated. Then, sensitivity was assessed by touching
the epiglottis, aryteÂnoid folds, and vocal cords with the tip of the
endoscope. During this phase, the presence of supraglottic and glottic
laryngeal injuries was recorded. Posterior commissure ulcers, which are common
due to the positioning of the endotracheal tube over the posterior glottic
commissure, were not considered for analysis.
For
the evaluation of saliva, the Murray scale16
was used, considering a grade 3 as a risk of aspiration.
Semi-solid and blue-colored liquid foods were then administered in three
different volumes: 5, 10, and 15 ml, recording each consistency with the
penetration-aspiration scale (PAS).17 The PAS scale
was stratified as follows for analysis: a score of 1, where the material does
not enter the airway, was considered normal (score 1); scores 2 to 5
(penetration) were grouped and given a value of 2 (score 2), and scores 6 to 8
(aspiration) were grouped with a value of 3 (score 3). Patients who did not
complete the food test due to high aspiration risk, difficulty performing
swallowing tasks, or inability to follow simple commands were given a score of
0 (zero), and these patients were considered to have dysphagia. Therefore,
patients with scores of 0, 2, and 3 were considered to have dysphagia.
Additionally,
a trans-tracheostomy evaluation was performed by removing the TQT cannula and
inserting the endoscope through the stoma in a cephalic direction to observe
the subglottic region and the inferior surface of the vocal cords. This method
was used to assess the presence of subglottic lesions.
The
study was recorded for review by the evaluation team, and the data were entered
into a database for subÂsequent analysis.
Patients
diagnosed with dysphagia received treatment until resolution and/or hospital
discharge. Those patients who still had dysphagia at the time of hospital
discharge were reevaluated through clinical assessment and/or video fluoroscopy
to document this variable.
Statistical analysis
Continuous
variables that assumed a normal distribution were reported as mean and standard
deviation (SD). Otherwise, the median and interquartile range (IQR) were used.
To determine the sample distribution of continuous variables, statistical tests
(Shapiro-Wilk test) and graphical methods (histograms and quantile-quantile
plots) were used. Two groups were formed based on the presence or absence of
dysphagia, as evaluated instrumentally through the FEES. To compare continuous
variables, the Student’s t-test or the Mann-Whitney U test was used, as
appropriate. For the comparison of categorical variables, the Chi-square test
or Fisher’s exact test was used, as appropriate. A p-value <0.05 was
considered significant. Data analysis was performed using IBM SPSS for
Macintosh, version 26.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Sample characteristics
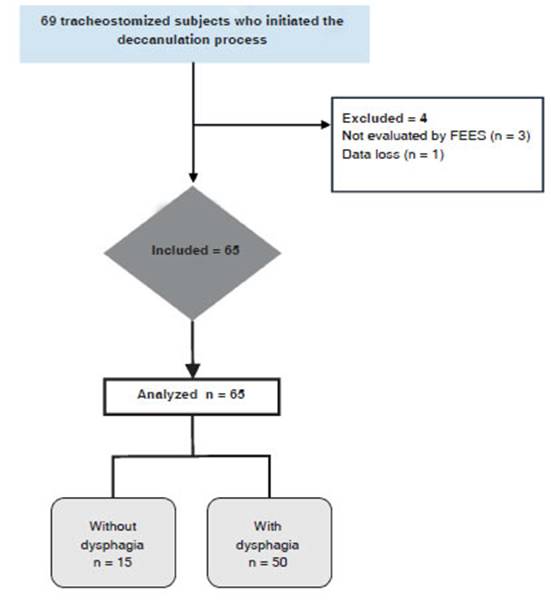
A
total of 69 tracheostomized patients undergoÂing decannulation were included in
the study. 4 subjects were excluded for the following reasons: 1 for data loss
and 3 for not having been evaluated by the FEES. (Figure 1)
Dysphagia
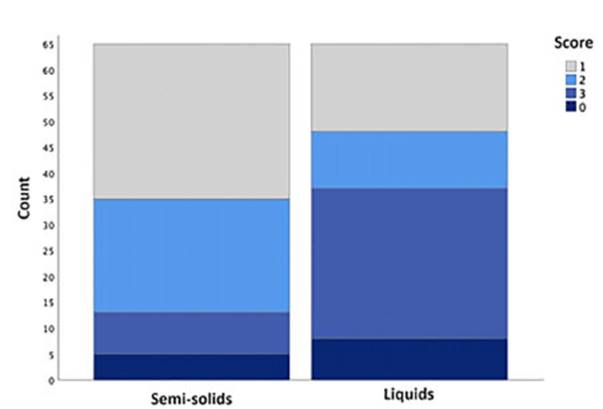
A
total of 65 patients were evaluated with the FEES, 50 of which were categorized as havÂing dysphagia (76.9 %).
During the evaluation with semi-solids, dysphagia was observed in 34 subjects
(52.3 %); of the 55 patients evaluated with this consistency, 6 (10.9 %)
presented silent aspiration. During the evaluation with liquids, dysphagia was
observed in 47 subjects (72.3 %). Of the 57 patients evaluated with liqÂuids,
17 (29.82 %) presented silent aspiration. Figure 2 shows the frequency
of dysphagia with the consistencies evaluated.
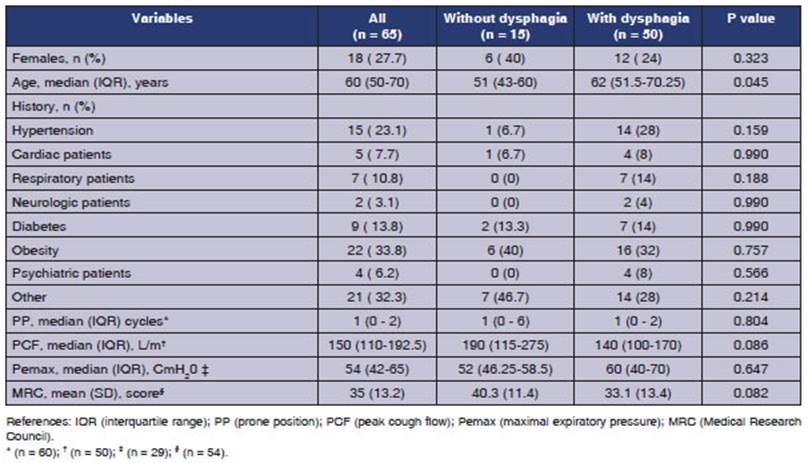
In
relation to the evaluation of the presence of saliva, the median score on the
Murray saliva scale was 1 point (IQR 1-2). In the group without dysÂphagia, it
was 1 point (IQR 0-1), and in the group with dysphagia, it was 1 point (IQR
1-2) (p=0.009).
The
median age of patients without dysphagia was 51 years (IQR 43-60), while for
those with dysÂphagia, it was 62 years (IQR 51.5-70.25) (p=0.045).
The
median number of days of IMV was 40.5 (IQR 32.25-48). Comparing the days of IMV
beÂtween the group without dysphagia [median 41 days (IQR 29-46)] and the group
with dysphagia [median 40 days (IQR 32-48)], no statistically significant
differences were observed between the two groups (p=0.726).
The
median number of days of OTI was 18 (IQR 16.5-21.5). Comparing the days of OTI
beÂtween the group without dysphagia [median 20 days (IQR 17-27)] and the group
with dysphagia [median 18 days (IQR 15-21)], no statistically significant
differences were observed between the two groups (p=0.14).
The
median number of days of TQT was 32 (IQR 21-60.5). Comparing the days of TQT
between the group without dysphagia [median 21 days (IQR 17-33)] and the group
with dysphagia [median 36 days (IQR 21 - 63.75)], statistically significant
differences were observed between the two groups (p=0.015).
Relationship between
the length of stay in the ICU and dysphagia
The
median number of days in the ICU was 48 (IQR 38-68.5). Comparing the days of
ICU between the group without dysphagia [median 51 days (IQR 37- 53)] and the
group with dysphagia [median 47.5 days (IQR 38-84.5)], no statistically
significant differences were observed between the two groups (p=0.544).
Relationship between
the duration of the decannulation process and dysphagia
Regarding
the days from the first result of the blue dye test to the removal of the TQT
cannula, information was obtained for a total of 61 subjects. The median number
of days of the decannulation process was 7 days (IQR 3.5-30). In patients withÂout
dysphagia, the median number of days until decannulation was 4.5 days (IQR 3 -
7), compared to 11 days (IQR 4-34) days in the group with dysÂphagia, showing a
statistically significant differÂence between the two groups (p=0.017).
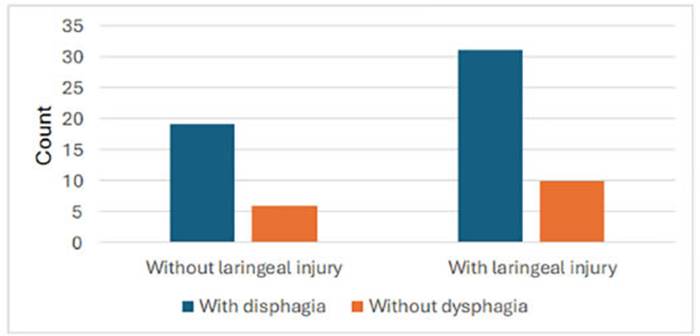
Laryngeal injury
A
total of 41 patients (63.1 %) showed at least one laryngeal injury. Of the 41
cases with laryngeal injury, 31 (75.6 %) had dysphagia, and of the 24 cases
without laryngeal injury, 19 (79.2 %) had dysphagia. This relationship was not
statistically significant (p=0.74) (Figure 3).
Decannulation failure
and dysphagia upon hospital discharge
Two
patients failed decannulation (3.07 %). One patient had to undergo a new
tracheostomy three weeks after decannulation due to bilateral vocal cord
paralysis. One patient required the placement of a Montgomery T-tube due to
subglottic stenosis.
At
the time of hospital discharge, a swallowing reevaluation was performed on 63
subjects. DysÂphagia persisted in twelve of them (19 %).
DISCUSSION
76.9
% of tracheostomized patients with COVID-19 presented with dysphagia for
semi-solid and/or liqÂuid consistency at the time of the endoscopic evaluÂation
of swallowing, prior to decannulation. These results are consistent with those
of other studies where dysphagia was evidenced using the FEES.18,19
The prevalence of dysphagia was higher with liquids than with semi-solids,
possibly because liquids require greater coordination and synchrony during the
pharyngeal stage of swallowing.
Among
the patients who could be evaluated with food and showed aspiration, a
considerable percentage corresponded to silent aspiration (PAS scale: 8
points). It was 11 % for semi-solid consisÂtency and 30 % for thin liquids.
Studies published by Sandblom and Boggiano et al report higher rates of silent
aspiration in these cohorts with COVID-19 and TQT.18,19
We
believe this may be due to the sensory alteraÂtions that occur in
tracheostomized patients. In this regard, the use of the FEES plays a key role
in the timely detection of these events, guiding the rehabilitation plan.
Dysphagia
is a common comorbidity followÂing critical illness associated with
malnutrition, increased risk of aspiration and pneumonia, lonÂger ICU stays,
compromised quality of life, and increased long-term mortality risk.21
Specifically,
in tracheostomized patients, the prevalence of dysphagia prior to the pandemic
ranged widely from 11 % to 93 %.12
This
frequency variability is due to the different evaluation methods used, the
criteria for defining dysphagia, and the heterogeneity of the patient
populations under evaluation.19 Therefore, it is difficult to
compare the prevalence of dysphagia in this cohort of COVID-19 patients with
previous data being so variable.
The
relationship between dysphagia and TQT remains a topic of controversy.
Available evidence indicates that dysphagia is common in tracheostoÂmized
patients, but it does not allow us to infer a causal relationship.12
There are factors related to the underlying disease or the reason for the TQT,
and factors triggered by the presence of an AA, muscle disuse atrophy,
disorders in the coordinaÂtion of breathing and swallowing, alterations in the
level of consciousness, all of which impact the airway protection mechanisms.21
We assume that apart from these factors there are the effects of the
COVID-19 virus on the central and periphÂeral nervous systems, where it has
been reported that it could affect sensory and motor functions linked to the
swallowing function. Future research is necessary to determine the true impact
of the SARS-CoV-2 virus within the physiopathological mechanism of
oropharyngeal dysphagia.22,23
In
our study, the median age was 60 years with a higher percentage of male sex,
and a median of 18 days of OTI, similar to the reported data.24,25
Arterial hypertension and obesity were the most prevalent comorbidities, as
reported by the study conducted in Argentina by
Estenssoro et al.9
We
observed a statistically significant difference in the age of the patients when
comparing the group with and without dysphagia. The prevalence of swallowing
disorders increases with age due to the natural aging process on the
oropharyngoÂlaryngeal structures.26 In elderly tracheostomized
patients, functional reserve and the number of days of TQT should be considered
as important factors when evaluating the oral intake, as it was evidenced that
tracheostomized patients over 70 years old take longer to achieve a safe
swallowing process.21 In the study by González Lindh et al,
similar results were observed in patients with very similar ages (64 vs. 53),
not being able to demÂonstrate a significant association between these
differences in age range and dysphagia.27
In
our study, patients with more TQT days were associated with the presence of
dysphagia (36 vs. 21 days; p: 0.015 %). Lindh et al observed similar results in
a series of 14 patients with COVID-19; although dysphagia was diagnosed
clinically.27 On the other hand, in a series of non-neurological
critically ill patients, Romero et al reported that the group with dysphagia
experienced a significant delay in the removal of the TQT cannula (50+/- 12 vs.
31+/-20; p= 0.01). The interesting aspect of this study is that it demonstrates
the presence of dysphagia evaluated through the FEES, even at the beginning of
the decannulation process.28 As mentioned previously, we cannot
establish an association or causality, but when dysphagia is present, it could
somehow influence the number of TQT days.
Of
the 41 patients who showed laryngeal injuries through the FEES,31 (75.6 %) had
dysphagia. We did not find a statistically significant associaÂtion between
laryngeal injuries and the presence of dysphagia, coinciding with the results
of our previous study.29 In the study by Rohuani et al, an
association was found between laryngeal injuries evaluated by the FEES and
swallowing abnormaliÂties using the self-administered EAT 10 (Eating
Assessment Tool) questionnaire.30 We consider that laryngeal
injuries would affect swallowing safety in terms of penetration and/or
aspiration.
The
decannulation failure rate was 3.07 % (n=2/65), similar to that reported in the
multiÂcenter Argentine study DECANULAR conducted on a heterogeneous sample of
patients.31 One of these patients required OTI and connection to IMV
due to poor secretion management, and one patient required a new tracheostomy
as a consequence of an airway injury. We have not found other research
evaluating decannulation failure in COVID-19.
In
our study, 19 % of patients presented with dysphagia at the time of hospital
discharge, similar to the results reported by the Boggiano study.19
These patients were followed up on an outpatient basis and via
telecommunication until their dysÂphagia resolved.
As
limitations of our study, we can mention that we were unable to access the
necessary data to calculate the total percentage of COVID-19 patients requiring
TQT in the ICU of our instituÂtion. Therefore, only the subgroup of patients
who successfully disconnected from mechanical ventilaÂtion and followed the
decannulation protocol was analyzed.
CONCLUSION
Oropharyngeal
dysphagia was prevalent in this cohort of COVID-19 patients. A significant
associaÂtion was found between patients with more TQT days until decannulation
and the development of dysphagia. The use of an instrumental assessment method
allowed us to make an early diagnosis and plan the treatment individually.
Conflict
of interest
Authors
have no conflicts of interest to declare.
REFERENCES
1.
Abe T, for the LUNG-SAFE Investigators and the ESICM Trials Group, Madotto F,
Pham T, Nagata I, Uchida M, et al. Epidemiology and patterns of tracheostomy
practice in patients with acute respiratory distress syndrome in ICUs across 50
countries. Crit Care [Internet]. 2018;22(1). http://dx.doi.org/10.1186/s13054-018-2126-6
2.
Frutos-Vivar F, Esteban A, Apezteguía C, et al. Outcome of mechanically
ventilated patients who require a tracheÂostomy. Crit Care Med [Internet]. 2005;33:290-8. http://dx.doi.org/10.1097/01.ccm.0000150026.85210.13
3.
Mahmood K, Wahidi MM. The changing role for tracheÂostomy in patients requiring
mechanical ventilation. Clin Chest Med [Internet]. 2016;37:741-51.
http://dx.doi.org/10.1016/j.ccm.2016.07.013
4.
Freeman BD. Tracheostomy update. Crit Care Clin [Internet]. 2017;33:311-22.
http://dx.doi.org/10.1016/j.ccc.2016.12.007
5.
Spiteri G, Fielding J, Diercke M. First cases of coronaÂvirus disease 2019
(COVID-19) in the WHO European Region. Euro Surveill [Internet]. 2020;25(9).
http://dx.doi.org/10.2807/15607917.ES.2020.25.9
6.
Ríos F, Risso-Vázquez A, Ballve D. Enfermedad por coronaÂvirus
2019 (COVID-19) aspectos de interés para cuidados críticos.:
Revisión narrativa. RATI. Disponible en: //revista.sati.org.ar/index.php/MI/article/view/698.
7.
Hosey MM, Needham DM. Survivorship after COVID-19 ICU stay. Nat Rev Dis Primers
[Internet]. 2020;6:60. http://
dx.doi.org/10.1038/s41572-020-0201-1
8.
Williams T, McGrath BA. Tracheostomy for COVID-19: evolving best practice. Crit
Care [Internet]. 2021;25(1). http://dx.doi.org/10.1186/s13054-021-03674-7
9.
Estenssoro E, Loudet CI, Ríos F. Clinical characteristics and outcomes
of invasively ventilated patients with COVID-19 in Argentina
(SATICOVID): a prospective, multicentre cohort study. The Lancet Respiratory
MediÂcine [Internet]. 2021;9:989-98.
http://dx.doi.org/10.1016/S2213-2600(21)002290
10.
Skoretz SA, Riopelle SJ, Wellman L, Dawson C. InvestigatÂing swallowing and
tracheostomy following critical illness: A scoping review. Crit Care Med
[Internet]. 2020;48:e141- 51.
http://dx.doi.org/10.1097/ccm.0000000000004098
11.
Gregoretti C, Pisani L. Tracheostomy, swallowing disorders and rehabilitation:
it is never too late. Minerva Anestesiol. 2015;81:357-9.
12.
Skoretz SA, Anger N, Wellman L, Takai O, Empey A. A systematic review of
tracheostomy modifications and swalÂlowing in adults. Dysphagia [Internet]. 2020;35:935-47. http://dx.doi.org/10.1007/s00455-020-10115-0
13.
Muhle P, Suntrup-Krueger S, Burkardt K, et al. StanÂdardized endoscopic
swallowing evaluation for TraÂcheostomy Decannulation in Critically Ill
Neurologic Patients - a prospective evaluation. Neurol Res Pract [Internet].
2021;3(1). http://dx.doi.org/10.1186/s42466-021-00124-1
14.
Benjapornlert P, Kagaya H, Shibata S, et al. The prevalence and findings of
fibre-optic endoscopic evaluation of swalÂlowing in hospitalised patients with
dysphagia. J Oral ReÂhabil [Internet]. 2020;47:983-8.
http://dx.doi.org/10.1111/joor.13026
15.
Langmore SE. History of fiberoptic endoscopic evaluation of swallowing for
evaluation and management of pharyngeal dysphagia: Changes over the years.
Dysphagia [Internet]. 2017;32:27–38. http://dx.doi.org/10.1007/s00455-016-9775-x
16.
Murray J, Langmore SE, Ginsberg S, Dostie A. The sigÂnificance of accumulated
oropharyngeal secretions and swallowing frequency in predicting aspiration.
Dysphagia [Internet]. 1996;11:99-103.
http://dx.doi.org/10.1007/bf00417898
17.
Butler SG, Markley L, Sanders B, Stuart A. ReliabilÂity of the Penetration
Aspiration Scale with flexible endoscopic evaluation of swallowing. Ann Otol
Rhinol Laryngol [Internet]. 2015;124:480-3.
http://dx.doi.org/10.1177/0003489414566267
18.
Osbeck Sandblom H, Dotevall H, Svennerholm K, Tuomi L, Finizia C.
Characterization of dysphagia and larynÂgeal findings in COVID-19 patients
treated in the ICU - An observational clinical study. PLoS One [Internet].
2021;16:e0252347. http://dx.doi.org/10.1371/journal.pone.0252347
19.
Boggiano S, Williams T, Gill SE, et al. MultidisciÂplinary management of
laryngeal pathology idenÂtified in patients with COVID-19 following
trans-laryngeal intubation and tracheostomy. J Intensive Care Soc [Internet]. 2022;23:425-32. http://dx.doi.org/10.1177/17511437211034699
20.
Zuercher P, Moret CS, Dziewas R, Schefold JC. Dysphagia in the intensive care
unit: epidemiology, mechanisms, and clinical management. Crit Care [Internet].
2019;23(1). http://dx.doi.org/10.1186/s13054-019-2400-2
21.
Pryor L, Ward E, Cornwell P, O’Connor S, Chapman M. Patterns of return to oral
intake and decannulation post-tracheostomy across clinical populations in an
acute inpatient setting: Oral intake and decannulation post-tracheostomy. Int J
Lang Commun Disord [InterÂnet]. 2016;51:556-67.
http://dx.doi.org/10.1111/1460- 6984.12231
22.
Aoyagi Y, Inamoto Y, Shibata S, Kagaya H, Otaka Y, Saitoh E. Clinical
Manifestation, Evaluation and RehabilitaÂtive Strategy of Dysphagia Associated
with COVID-19. Am J Phys Med Rehabil. 2021;100:424-31.
http://dx.doi.org/10.1097/PHM.0000000000001735.
23.
Li Z, Liu T, Yang N, Han D, Mi X, Li Y, et al. Neurological manifestations of
patients with COVID-19: potential routes of SARS-CoV-2 neuroinvasion from the
periphery to the brain. Front Med [Internet]. 2020;14:533-41.
http://dx.doi.org/10.1007/s11684-020-0786-5
24.
Chao TN, Harbison SP, Braslow BM, et al. Outcomes after tracheostomy in
COVID-19 patients. Ann Surg [Internet]. 2020;272:e181-6.
http://dx.doi.org/10.1097/sla.0000000000004166
25.
Tornari C, Surda P, Takhar A, et al. Tracheostomy, ventilaÂtory wean, and
decannulation in COVID-19 patients. Eur Arch Otorhinolaryngol [Internet]. 2021;278:1595-604.
http://dx.doi.org/10.1007/s00405-020-06187-1
26.
Cichero J. Age-related changes to eating and swallowÂing impact frailty:
Aspiration, choking risk, modified food texture and autonomy of choice.
Geriatrics (Basel) [Internet]. 2018;3:69.
http://dx.doi.org/10.3390/geriatÂrics3040069
27.
Lindh MG, Mattsson G, Koyi H, Johansson MB, Razmi R, Palm A. Swallowing
function in COVID-19 patients after invasive mechanical ventilation. Arch
Rehabil Res Clin Transl [Internet]. 2022;4:100177.
http://dx.doi.org/10.1016/j.arrct.2021.100177
28.
Romero CM, Marambio A, Larrondo J, Walker K, Lira M-T, Tobar E, et al.
Swallowing dysfunction in nonneurologic critically ill patients who require
percutaneous dilatational tracheostomy. Chest [Internet]. 2010;137:1278-82.
http://dx.doi.org/10.1378/chest.09-2792
29.
Chiappero G, Falduti A, Catini ME, Raimondi N. Evaluación
endoscópica de la deglución: Una necesidad creciente en terapia
intensiva. Rev Argent Terap Intens. 2018;35(2).
30.
Rouhani MJ, Clunie G, Thong G, et al. A prospective study of voice, swallow,
and airway outcomes following tracheosÂtomy for COVID-19. Laryngoscope
[Internet]. 2021;131(6). http://dx.doi.org/10.1002/lary.29346
31.
Diaz Ballve P, Villalba D, Andreu M. Factores predictores de dificultad para la
decanulación. Estudio de cohorte multicéntrico. Rev Am Med Resp. 2017;1:12-24.

| GalerĂa de imágenes | ||
| Mujer joven con afectaciĂłn pulmonar bilateral y alteraciĂłn de la conciencia | ||
Autores: Churin Lisandro |
 |
|