

Autor : Vegetti, Luciana1, Ballina, Ariel1, Wustten, SebastiÃĄn1, Maillo, MartÃn1, Gonzalo, Paula1, GonzÃĄlez Vara MartÃn1 Guala Eugenia1, Altamirano, Agustina1, Bima, Guillermo1, Di Rienzo, Paula1, Lombardi, MarÃa Rosa1, MonzÃģn, VerÃģnica1, Bringas, Liset1, Saint Paul, Evangelina2, Varino, NicolÃĄs3, Ãlvarez Padilla, Facundo N4
1Pulmonology and Allergy Service, Hospital JosÃĐ MarÃa Cullen, Center of Outpatient Medical Specialties of Santa Fe. (CEMAFE) Argentina.
2Oncology. Thoracic Oncology Group, CEMAFE.
3Biostatistics Services, Hospital Cullen.
4Thoracic Surgery Division, Hospital JosÃĐ MarÃa Cullen. Thoracic Oncology Group, CEMAFE. Nursing, Pulmonology and Allergy, Hospital JosÃĐ MarÃa Cullen and CEMAFE.
https://doi.org./10.56538/ramr.NCNG2904
Correspondencia : lavegetti@hotmail.com. Luciana Vegetti
ABSTRACT
Lung
cancer (LC) is a neoplasm with a poor prognosis, it is the third leading cause
of cancer death and the highest mortality worldwide.
The
objective of the study is to describe the clinical characteristics of patients
diagnosed with lung cancer, evaluated over 21 years by the multidisciplinary
Committee of a hosÂpital in the city of Santa Fe, Argentina (MCLC) and the
comparative analysis between the first period from 2001 to 2011 (p1) and the
second (p2) between 2012 and 2022.
It
is a descriptive, observational and retrospective study. A total of 416 adult
patients of both sexes with a diagnosis of lung cancer between June 2001 and
July 2022 were studied, 211 patients in the first decade and 205 in the second.
65 patients with clinical radiological diagnosis of lung cancer were excluded
from the analysis.
The
results showed that 294 (70.7%) were male, with a mean age of 60 years. It was
observed that 249 patients (80.72%) suffered from one or more comorbidities and
the
most
frequent pathologies were 146 cases of COPD (58.9%, p: 0.05), 19 cases of diaÂbetes
(7.7%), 11 patients with chronic liver disease (5%), 23 cases with cardiac
disease (9.32%) and 10 patients with chronic kidney disease (4.3%).
Smoking
was recorded in 320 patients (81.3%) includes ex-smokers (66.7% of women and
87.1% of men) with a mean of 50 pack-years (3 to 169 p/y). Smoking in general
decreased at the expense of men, but there was an increase in smoking in women.
The
most frequent histology was adenocarcinoma with 149 cases (35.6%, p: 0.04),
followed by squamous or squamous cell carcinoma with 128 cases (30.8%, p:
0.04), 44 cases of small cell neuroendocrine carcinoma or oat cell (10.6%, p:
0.06), 65 undifÂferentiated (15.6%, p 0.05), 10 large cell carcinoma (2.4% p.
0.12), 7 carcinoid tumors (1.7%, p: 0.15) and other recorded histologies there
were 6 cases of mesothelioma (1.44%) and 7 (1.7%) extra tumors pulmonary.
It
is observed that in the second period adenocarcinoma increased significantly
from 32.7% to 39.02%, while for epidermoid the cases decreased from 40.7% to
32.8%. An increase from 9.45% to 21.46% was also established for
undifferentiated cases and in oat cell histological types no changes were seen
(10.9 to 10.2%).
The
most used diagnostic methods were bronchoscopy and puncture under CT. A total
of 172 endoscopies (41.7%) were performed, which had the highest performance in
the ca epidermoid and 110 °CT-guided punctures (26.7%) were performed, with the
highest diagnostic yield in adenocarcinoma.
For
staging, the TNM edition was used at the time of diagnosis, both sexes were in
advanced stages in the main strains of non- small cell neoplasms.
Ninety-two
patients (22%) received surgical treatment with curative intent, 292 patients
(70%) received cancer treatment based on chemotherapy and/or radiotherapy, and
33 patients (8%) received only palliative treatment.
Key
words:
Lung cancer; Histological types; Adenocarcinoma
RESUMEN
El
cáncer de pulmón es una neoplasia de mal pronóstico. Es la
tercera causa de muerte por cáncer y el de mayor mortalidad a nivel
mundial.
El
objetivo del estudio es describir las características clínicas de
los pacientes con diagnóstico de cáncer de pulmón,
evaluados a lo largo de 21 años por el Comité multiÂdisciplinario
de un hospital de la ciudad de Santa Fe, Argentina y el análisis
comparativo entre el primer período del 2001 al 2011 (P1) y el segundo
(P2) entre 2012 y 2022.
Es
un estudio descriptivo, observacional y retrospectivo. Se analizó un
total de 416 pacientes adultos, de ambos sexos con diagnóstico de
cáncer de pulmón comprenÂdidos entre junio 2001 a julio 2022, en
la primera década 211 pacientes y 205, en la segunda. Se excluyeron del
análisis 65 pacientes con diagnóstico clínico radiológico
de cáncer de pulmón.
Del
total de pacientes 294 (70,7%) eran varones, con edad media de 60 años.
Se
observó que 249 pacientes (80,72%) padecía una o más
comorbilidades y las patoÂlogías más frecuentes fueron 146 casos
de enfermedad pulmonar obstructiva crónica (58,9%, p = 0,05), 19
casos de diabetes (7,7%), 11 pacientes con hepatopatía crónica
(5%), 23 casos con patología cardíaca (9.32%) y 10 pacientes con
enfermedad renal crónica (4,3%).
El
tabaquismo se registró en 320 pacientes (81,3%) incluye a los
exfumadores (66,7% de las mujeres y 87,1% de los hombres) con una media de 50
paquetes/año (3 a 169 p/a). El tabaquismo en general disminuyó a
expensas de los hombres, pero se evidenció un incremento del
hábito tabáquico en las mujeres.
La
histología más frecuente fue el adenocarcinoma, con 149 casos
(35,6%, p = 0,04), seguidos del carcinoma escamoso o epidermoide, con
128 casos (30,8%, p = 0,04), 44 casos de carcinoma neuroendocrino de
pequeñas células u oat cell (10,6%, p = 0,06), 65
indiferenciados (15,6%, p = 0,05), 10 carcinomas de células
grandes (2,4% p = 0,12), 7 tumores carcinoides (1,7%, p = 0,15) y
otras histologías registradas fueron 6 casos de mesotelioma (1,44%) y 7
(1,7%) tumores extrapulmonares.
Se
observó que en el segundo período el adenocarcinoma
aumentó significativamente del 32,7% al 39,02%, mientras que, para
epidermoide, los casos descendieron de 40,7% a 32,8%. También se
estableció para los casos indiferenciados un incremento del 9,45% al
21,46% y en los tipos histológicos oat cell no se percibieron
cambios (10,9% al 10,2%).
Los
métodos diagnósticos más utilizados fueron la
broncofibroscopia y la punción bajo tomografía computarizada. Se
realizaron 172 endoscopias (41,7%) que fueron de mayor rendimiento en el
cáncer epidermoide y se realizaron 110 punciones guiadas por tomoÂgrafía
computarizada (26,7%), de mayor rendimiento diagnóstico en el
adenocarcinoma.91
Para
la estadificación se utilizó la edición TNM al momento del
diagnóstico, ambos sexos se encontraban en estadios avanzados en las
principales estirpes de neoplasias no células pequeñas.
Recibieron
tratamiento quirúrgico con intención curativa 92 pacientes (22%),
tratamiento oncológico a base de quimioterapia o radioterapia 292
pacientes (70%), y 33 pacientes (8%) recibieron tratamiento paliativo
único.
Palabras
claves: Cáncer
de pulmón; Tipos histológicos; Adenocarcinoma
Received: 08/27/2022
Accepted: 04/24/2022
INTRODUCTION
Lung
cancer (LC) is a malignancy with a poor prognosis. It is the most common cause
of cancer-related deaths, with the highest incidence and mortality worldwide,
accounting for 24% of deaths in men and 21% in women. LC represents an imÂportant
public health problem, with a progressive increase in mortality since the
beginning of the last century, which led to the first epidemiological studies linking
LC to tobacco use.1-5 In 2018, GLOÂBOCAN
(Global Cancer Observatory) estimated 2.09 million new cases (11.6% of all
cancer cases) and 1.76 million deaths (18.4% of total cancer deaths), making it
the most common cause of cancer-related deaths in both men and women.6 Its incidence
has significantly increased in women due to the rise in smoking habits among
them. If the current trend continues, it is estimated that by 2045, deaths from
LC in women will surpass those in men. Identified risk factors include smoking,
environmental factors, occupational factors, and biological and genetic factors
related to the host. The World Health Organization (WHO) estimates that 48% of
men and 10% of women globally are smokers. Up to 80% of current smokers live in
low- and middle-income countries, and more than half of lung cancer deaths
occur in less developed regions, likely due to limited access to healthcare
resources. The highest 5-year survival rate is obÂserved in the United States,
reaching 15%, while in Europe it is around 8%, similar to the one in countries
with lower economic development. Mean age: 70 years.1, 3, 4
In
Argentina, in 2018, cancer accounted for 19% of all causes of death, and among
malignant tumors, LC represented 16% of all cancer-related deaths, with a peak
in the 65-74 age group.
In
terms of gender, men were the most affected worldwide, with 68%, and 32% for
women. In our country, 73% of deaths from this type of cancer occurred in men.
However, LC mortality showed a significant decline in men from 2000 to 2015,
with an estimated annual percentage change (EAPC) of -1.7% for the entire
country. On the other hand, the trend in women was upward, with a significant
increase in EAPC of 2.5%.2
The
three most common histological subtypes are: adenocarcinoma, squamous cell
carcinoma, and small cell carcinoma. The declining trend in men was observed
for most subtypes except for adÂenocarcinoma, whereas in women, there continues
to be an increasing incidence in all the histological variants, although adenocarcinoma
is the most common. The decrease in tobacco consumption explains the lower
incidence of squamous cell carcinoma in men. However, the increasing inciÂdence
in women suggests different etiologies for the development of different
subtypes of LC. The prognosis, although generally poor, is not the same for all
subtypes.7, 8
The
study of lung cancer has shown that it is a heterogeneous tumor with several
types of difÂferentiation recognized by the WHO classification. This
heterogeneity has been addressed in many ways: histological, cellular, and
molecular/genetic, as it has a significant impact not only on tumor
classification but also on prognosis and treatment definition. The progressive
development of genetic and molecular studies helps determine treatment
strategies and improve prognosis.9
Given
these figures, it is indisputable that LC is a real public health problem and a
challenge for healthcare teams. Prioritizing the importance of preventive
public health policies, encouraging early consultation in the presence of
symptoms, screening in smoking patients, and mostly adoptÂing a
multidisciplinary approach are crucial, given that early diagnosis offers the
possibility of surgiÂcal treatment and subsequent follow-up, resulting in
improved survival.
OBJECTIVE
To
analyze the lung cancer situation in a referÂence hospital in the city of Santa
Fe over a 21-year period of data collection in a multidisciplinary committee.
The clinical, histological, and epideÂmiological characteristics of patients
diagnosed with lung cancer are described. The changes in two 10-year periods of
different subtypes of lung cancer are compared, along with their relationship
with different risk factors and their diagnostic and treatment methods.
MATERIALS AND METHODS
Descriptive,
observational and retrospective study. A total of 416 adult patients of both
sexes diagnosed with lung cancer were studied encompassing the 21 years of
operation of the MCLC (Multidisciplinary Committee on Lung Cancer), from June
2001 to July 2022.
In
addition to examining general data, analyses were conducted during two periods:
2001-2011 (P1) and 2012- 2022 (P2).
The
studied variables included: patientsâ gender and age, smoking index, patientsâ
comorbidities, diagnostic procedures performed, and therapeutic approach
applied. Regarding the variables related to the neoplasm, the foÂllowing data
were recorded: diagnosis date, histological type, and cancer stage at the time
of diagnosis according to the TNM classification.
The
histological subtypes were defined based on morÂphology and
immunohistochemistry as adenocarcinoma, squamous cell carcinoma, small cell
carcinoma, large cell carcinoma, undifferentiated carcinoma, carcinoid tumor,
mesothelioma, and others. Only histological groups with a higher number of
patients were included in the statistical analysis: adenocarcinoma, squamous
cell carcinoma, undiÂfferentiated carcinoma, and small cell carcinoma.
For
the statistical analysis of the data in general, summary measures of
distribution, including frequency, measures of central tendency, and measures
of data disÂpersion, were first established. Furthermore, regarding the
comparison of frequency of cases by their groups, measures of association and
comparison between population subÂgroups were established. Confidence intervals
for means and proportions were also established, along with odds ratios, aiming
to determine potential impact measures on the variation between period P1 and
P2.
RESULTS
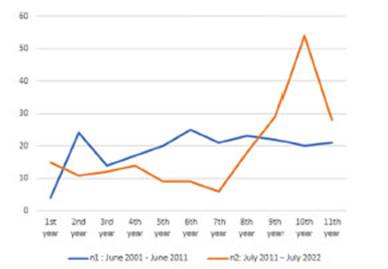
Between
June 2001 and July 2022, a total of 416 adult patients of both sexes diagnosed
with lung cancer were admitted to Hospital Cullen in the city of Santa Fe. The
comparison between the two 10-year periods showed 211 patients in the first
period and 205 in the second period (Figure 1).
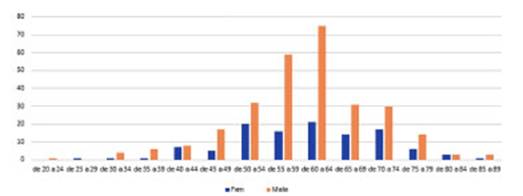
The
mean Âą standard deviation of the number of patients diagnosed with lung cancer
per year was 18.9 Âą 10.38 (range 4 to 54 cases, mean 18.8 cases) (Figure 2).
The
annual presentation of cases remained stable over the years, with an increase
observed from 2020 when the committee switched to virtual
meetings due to the pandemic. The number of participating doctors
increased, and the weekly frequency was maintained.
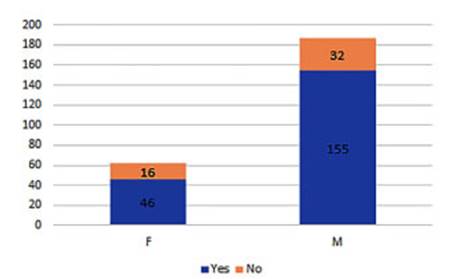
Out
of the total patients, 294 were male (70.7%) and 122 were female (29.3%),
resulting in a male-to-female ratio of 2.4:1. Mean age was 60 Âą 10 (range: 22 -
89) and no significant changes were observed in this variable throughout the
study period (p 0.04).
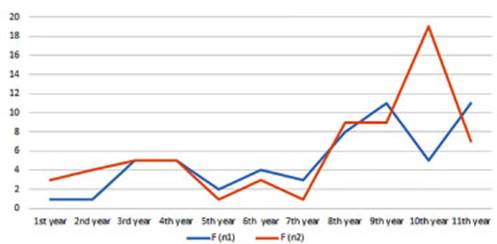
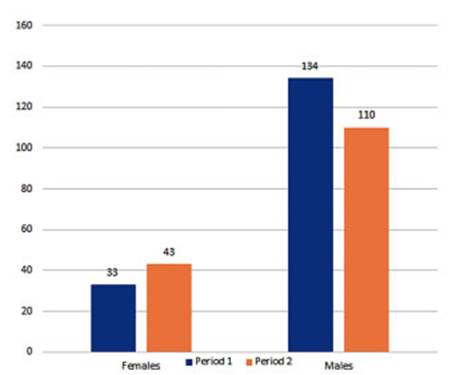
In
terms of gender, in the last decade, there was an increase in the diagnosis of
lung cancer in women, from 56 to 66 cases, accounting for a 6% increase
(chi-square value of 1.34 and p-value of 0.24; so we can say that this
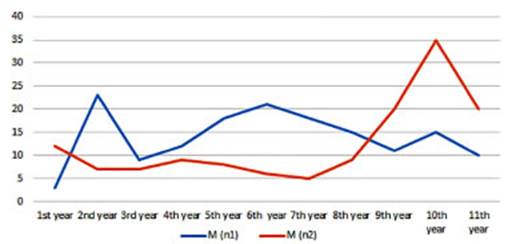
variation is indepenÂdent between the two periods) (Figure 3). In men, there
was a significant decrease in the diagnosis, from 156 cases in P1 to 138 in P2,
representing a 6% decline in cases between periods (p 0.06, odds ratio: 0.75,
95% CI between 124 and 151 cases) (Figure 4).
70%
percent of the patients fell within the age range of 50 to 70 years. For P1,
the mean age was 60 years (range: 32 to 89 years), and 50% of the population
was between 54 and 65 years old. In contrast, for P2, the mean age was 62 years
(range: 22 to 88 years), with 25% of 55 years and 75% of 70 years. (Figure 2).
In
the study of medical history (known comorÂbidities), 249 patients were
registered, with one or more comorbidities observed in 80.72% (95% CI 75.27% -
85.43%). 82.9% of men and 74.2% of women had one or more comorbidities (p
0.132). The most common disease was COPD (159 cases) (58.9% of the registered
cases, 95% CI between 53% and 65%); and the other comorbidities accounted for
the following percentages: 7.7% (19 cases) of diabetes, 5% (11 cases) of liver
disease, 9.32% (23 cases) of heart failure, and 4.3% (10 cases) of renal
failure (Figure 5). The cases of women diagnosed with COPD decreased from 71%
in P1 to 32.5% in P2 (significant variation according to a chi-square value
with one degree of freedom, resulting in p: 0.001). On the other hand, men
diagnosed with COPD showed a decrease from 78.2% in P1 to 41.3% in P2 (p
greater than 0.5).
With
regard to smoking, 320 patients reported being smokers (80.96%), including
former smokÂers, and 74 (18.78%) had never smoked. When evaluated by sex, 87.1%
of men and 66.67% of women were smokers (p: p: 0.047). The mean number of packs
per year in smokers was 49.34 +/- 26.1. In the case of men, it was 53.04 +/-
27.37, and in women, it was 37.52 +/- 17.59. (Figure 6).
The
most frequent age group was between 54 and 64 years old, with 51.1% of smokers falling
within this range. In the comparison of periods, no significant variations in
overall tobacco consumpÂtion were observed, with approximately 80% of the cases
remaining consistent. Smoking in general decreased in men, and there was an
increase in the smoking habit in women. In P1, 62.26% of women were smokers (p:
(p: 0.067), and in P2, it increased to 70.5% (p: 0.02). (according to the
chi-square value of 0.863 calculated for this variation with one degree of
freedom, the probability is greater than p: 0.35, indicating a statistically
insignificant independent variation). Among men, there was a decrease in
smoking habits from P1, with 88.7%, to P2, with 84.5%, which was not
statistically significant.
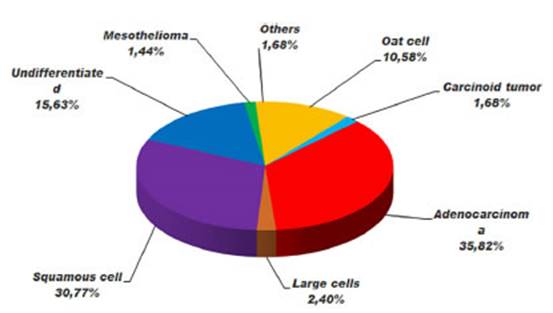
The
analysis of tumor strains revealed that the most frequent histology was
adenocarcinoma with 149 cases (35%, p: 0.04), followed by squamous cell
carcinoma with 128 cases (30.8%, p: p: 0.04). The remaining histological
variants were distributed as follows: 44 small cell neuroendocrine carcinomas
(10.58%, p: 0.06), 65 undifferentiated carcinomas (15.6%, p: 0.05), 10 large
cell carcinomas (2.4%, p: 0.12), 7 typical carcinoid tumors (1.7%, p: 0.05);
and other recorded histology types included 6 mesotheliomas (1.6%) and 7
isolated cases (1.7%) of extrapulmonary tumors (thymoma, low-grade
mucoepidermoid tumor, sarcoma, lymphomas, ovarian granulosa cell tumor) (Figure
7).
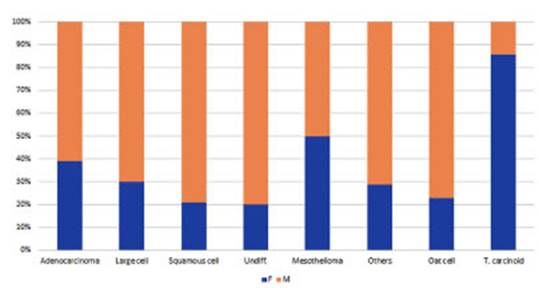
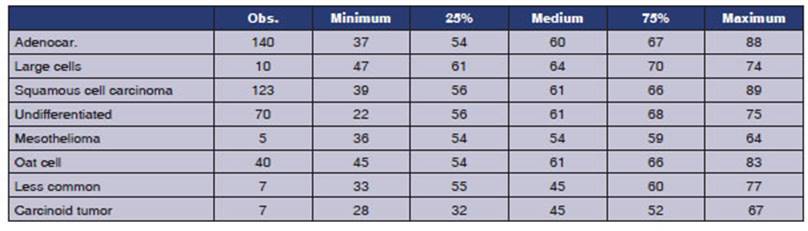
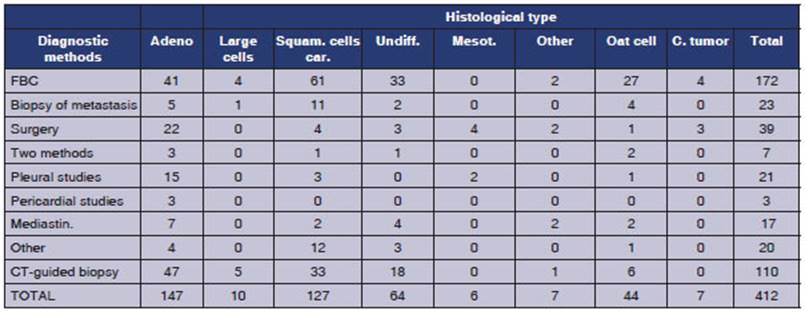
The
male-to-female ratio varies depending on the tumor strains: males generally
predominate except for carcinoid tumors, which had 6 cases in females and 1
case in a male. In adenocarcinoma, 60.8% are men (p: 0.001), while in squamous
cell carcinoma, 78.9% are men (p: 0.0139). For large cell tumors, 70% are men,
and for small cell tuÂmors, men account for 77.3% ( p:
0.3). Among the 6 cases of mesothelioma that have been registered, there is an
equal number of men and women (Figure 8). The mean age is 60 years, except for
carcinoid tumors that occurred in much younger women. (Table 1)
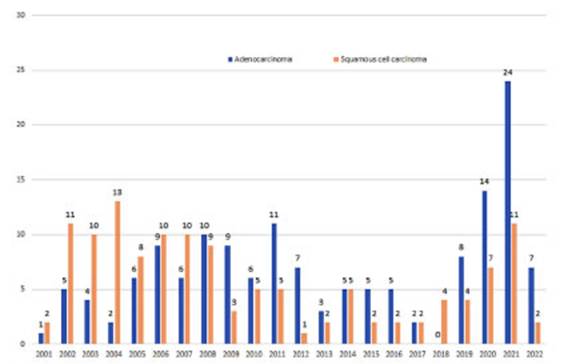
The
behavior exhibited by the adenocarcinoma is very interesting, with a gradual
frequency inÂcrease starting from 2005 until it surpassed the squamous cell
carcinoma in 2008, and remaining as the most commonly diagnosed histology, exÂcept
in 2018 when only 6 tumors were recorded (4 squamous cell carcinomas, 1
undifferentiated, and 1 small cell carcinoma). It is assumed that no
adenocarcinoma was observed due to underreportÂing of presented patients
(Figure 9).
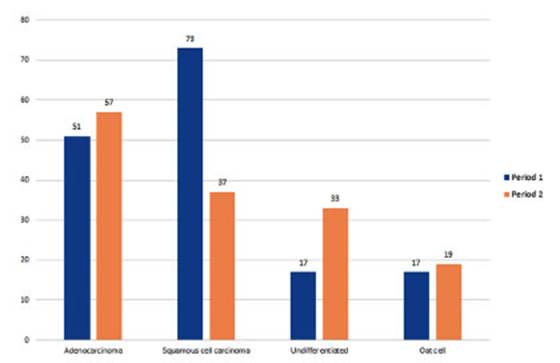
The
most common strain in smokers was squaÂmous cell carcinoma (110 cases).
According to the statistical analysis, it varied from 43.7% of cases at P1 (p:
0.0007) to 32.2% of cases at P2 p: 0.007). The second most common strain, with
a very small difference, was adenocarcinoma with 108 cases (p: 0.007).
Adenocarcinoma with 31 cases was the most common strain in non-smokers,
representing 41.9% of tumors diagnosed in non-smoking patients (p: 0.19). Among
non-smokers, 51.6% of adenocarcinoma cases were women, with 16 cases: 9
patients at P1 and 7 at P2 (p: 0.013). Undifferentiated carcinoma in smokers
showed a growth from 10% to 21.7% in period 2 (chi-square test with 1 degree of
freedom yielded p: 0.0007) (Figure 10).
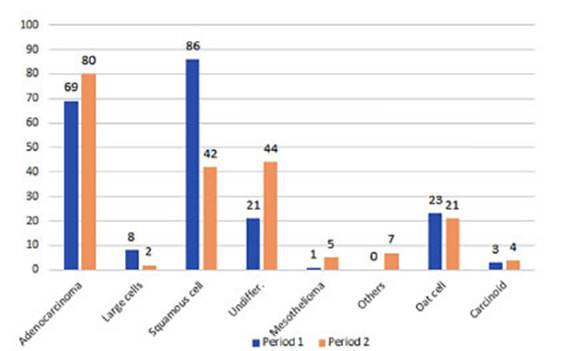
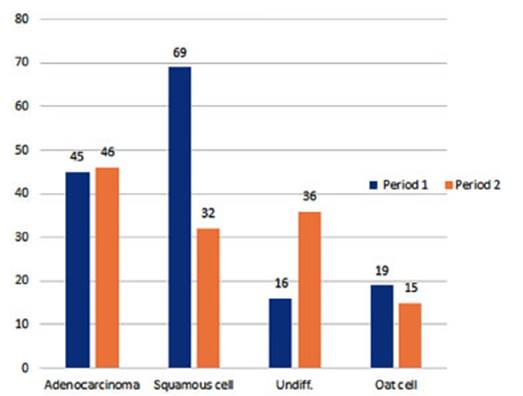
If
we analyze the data by periods, the numÂber of adenocarcinoma cases increased
from 69 (32.7%) in P1 to 80 (39%) in P2 (the variation is not significant, with
a chi-square value resulting in p: 0.17). The number of cases of squamous cell
carcinoma significantly decreased from 86 to 42 (40.7% to 20.4%, respectively).
(p: 0.000007). Undifferentiated tumors increased from 9.45% to 21.46% (p:
0.002). No changes were observed in oat cell histological types, (10.9% to
10.2% of cases in each period) (Figure 11).
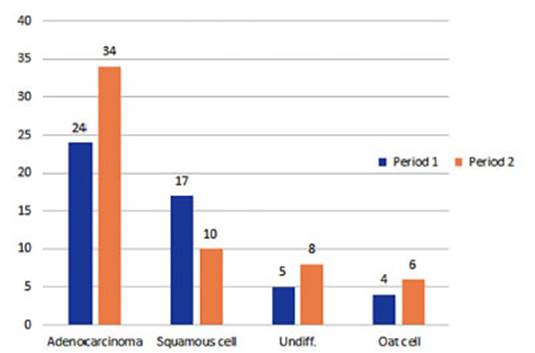
The
observed increase in adenocarcinoma cases appears to be related to a higher
number of diagÂnoses in women: in P1, there were 24 cases, which increased to
34 cases in P2 (from 42% to 51%). However, no statistical relationship was
found (p: 0.33), always considering the small number of patients. (Figure 12).
In the case of men, a clear negative variation is observed in the squamous cell
carcinoma strain, with cases decreasing from 69 to 32 in both periods
(representing a percentage change from 44.5% to 23%,
respectively, with a p-value of 0.0001) (Figure 13).
Regarding the undifferentiated strain, there appears to be an
apparent relationship with an increase in men. The number of cases went from 16
in P1 to 36 in P2 (from 10.3% to 25.9% of the cases). (p: 0.50). In the second
period, a total of 79 patients with undifferentiated carcinoma underwent
immunohistochemistry methods for further characterization. As a result, it was
deterÂmined that 38% of these tumors (30 cases) were adenocarcinoma, while
34.18% (27 cases) remained undifferentiated. If we focus on the last 3 years,
28 undifferentiated tumors were diagnosed, out of which 26 underwent
immunohistochemistry techniques. This allowed for the differentiation of the
morphology in 10 cases as squamous cell carcinoma, 7 cases as adenocarcinoma,
and 2 cases as undifferentiated carcinoma. 2 patients were diagnosed with
extrapulmonary tumors, 4 cases lacked documentation, and in 2 cases, the techÂniques
were not performed due to patient death.
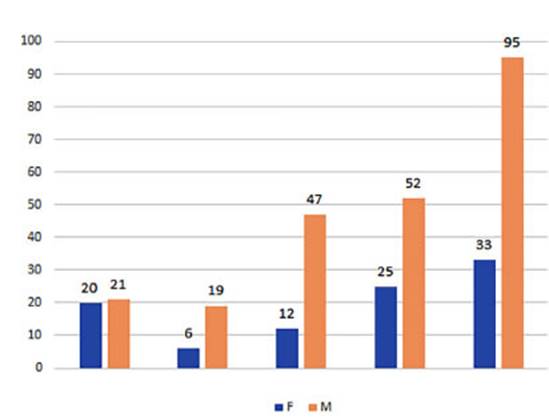
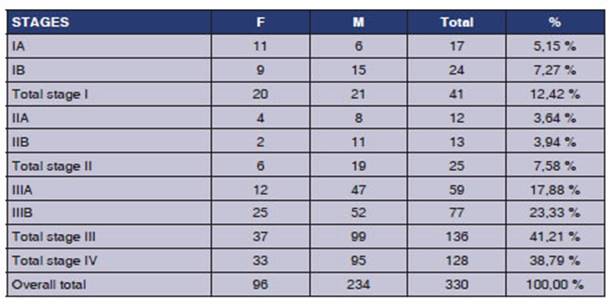
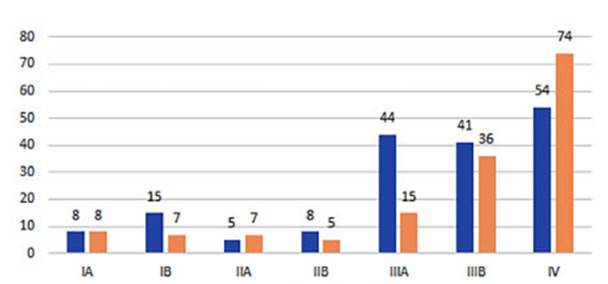
For the staging distribution, the TNM edition was used at the time
of patient diagnosis. The patients for whom TNM was determined totaled 330 (234
male and 96 female) and were distributed in stages (S). SI: 12.4%, SII: 7.58%,
SIIIA: 17.88%, SIIIB: 23.33% and SIV: 38.8%. (Figure 14, table 2).
The
majority of patients of both sexes were in advanced non-surgical stages at the
time of diagnosis.
One
of the significant findings we were able to provide was the fact that patients
diagnosed in stage IV increased from 30.8% in P1 to 47.7% in P2. (p: 0.001). On
the other hand, cases in stage IIIA decreased from 44 to 15 in the respective
periods (from 25.1% to 9.6%, p: 0.002). (Figure 15)
There
were 16 cases of patients in stage I who underwent curative surgery, and the
histological type in most of them was adenocarcinoma.
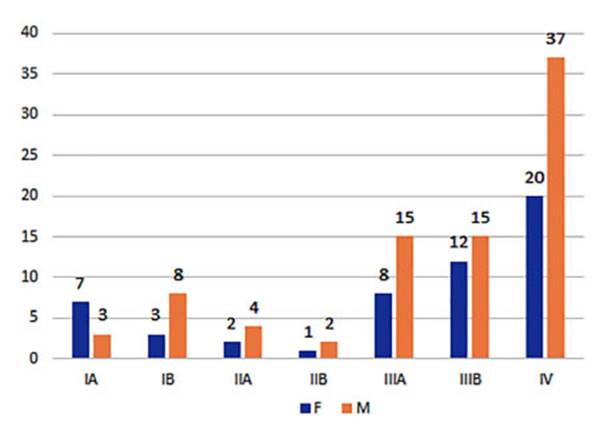
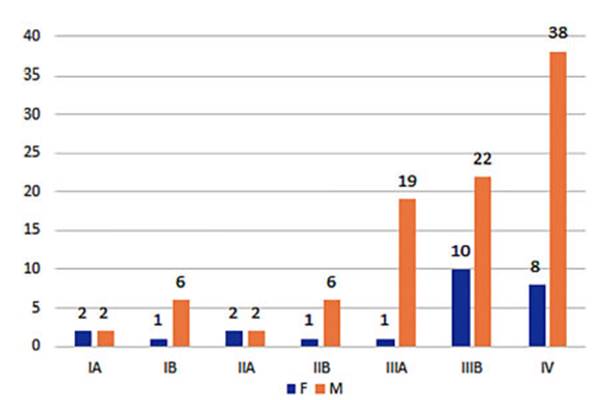
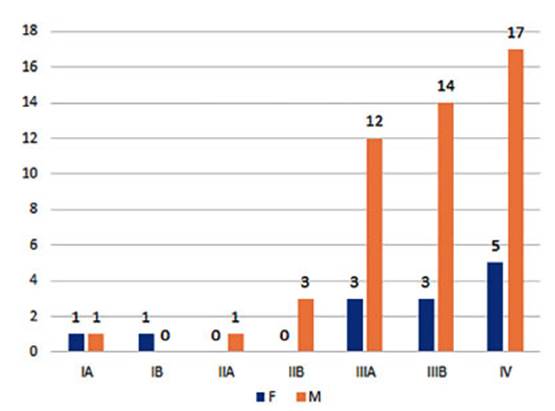
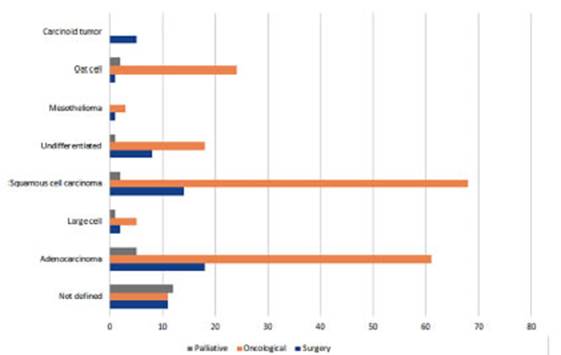
Regarding
the three analyzed histological types, it was also observed that they were in
advanced non-surgical stages (Figures 16 to 18).
Half
of the 65 patients with clinical and radioÂlogical diagnosis were in advanced
stage IV with poor performance status and did not undergo diÂagnostic methods
or treatment. For the remaining patients, histology data could not be
retrieved, so it was decided to exclude them from the patient group.
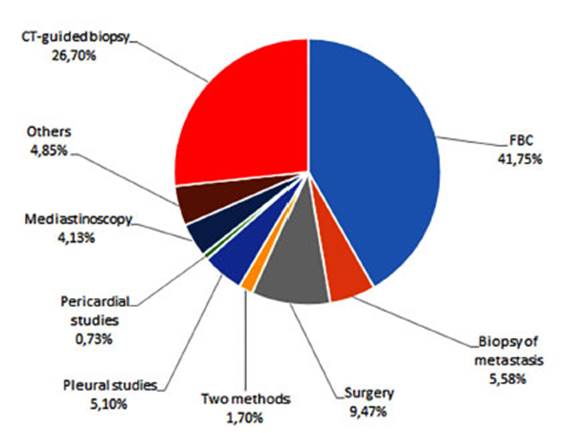
The
most commonly used diagnostic methods in our practice to determine the
histological strain were fiberoptic bronchoscopy and
CT-guided biÂopsy, followed by surgical methods (Figure 19). Other methods that
havenât been that common over the years included 9 radioscopy-guided biÂopsies
and 11 sputum cytologies, which are now obsolete. A total of 172 fiberoptic
bronchoscopies and 110 CT-guided biopsies were performed. When considering the
various surgical methods used to reach a histological diagnosis, the most
frequent were: 39 lung resection surgeries (for diagnosis/ treatment in early
stages), 21 pleural studies, and 3 pericardial studies (without specifying the
method), as well as 17 mediastinoscopies.
With regard to the location of the different strains, CT-guided
biopsy was more frequently used for adenocarcinoma, while fiberoptic bronÂchoscopy
was more commonly used for squamous cell carcinoma. (Table 3)
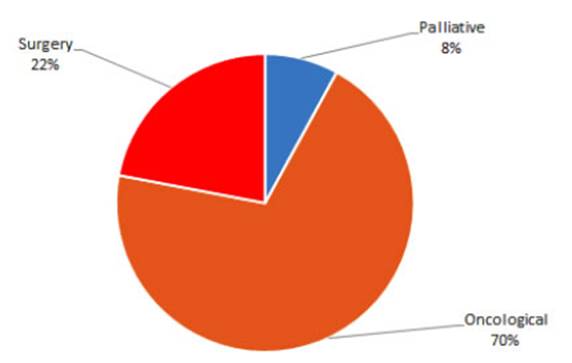
In terms of treatment, 92 patients (22%) reÂceived surgical
treatment with curative intent, 292 patients (70%) received oncological treatÂment
based on chemotherapy and/or radiation therapy, and 33 patients (8%) received
only palÂliative treatment due to their advanced condiÂtion and poor
performance status (PS) (Figures 20 and 21).
DISCUSSION
In
our study, we observed that out of the 416 patients diagnosed with lung cancer
over these 21 years at MCLC, 71% were male and 29% were female. When comparing
the two
decades, we noted a decrease in the number of cases in men and an
increase in women, but without statistical significance.
The mean age of 60 years is lower than the one reported in the
literature, and it did not vary over the years.1,3
Both men and women showed comorbidities in 80% of the cases. COPD
is the most prevalent condition, but we did not prioritize its staging.
Smoking is the leading cause related to lung cancer, with 81% of
our patients being smokÂers. It is predominant in both sexes, although more
prevalent in men, in accordance with the literature10.
The mean pack-years reached 51. Smoking itself has decreased over the years,
priÂmarily among men, while in women, the rate has increased significantly.
We did not prioritize the registration of occuÂpational exposure,
which is considered potentially risky for the development of lung cancer, so we
cannot describe any relationship.
The comparative analysis between the two decades confirms a shift
in the distribution of hisÂtological strains of lung cancer, with an increased
percentage of adenocarcinoma and a decrease in squamous cell carcinoma. In our
series, the inÂcrease in adenocarcinoma is associated with the female gender,
as it remained stable in men. UnÂlike the undifferentiated types that increased
in both sexes but more significantly in men, we were unable to conduct a complete
analysis of these subÂtypes with post-immunohistochemistry diagnosis since we
have records starting from the second decade, and most of this group would
possibly be cases of adenocarcinoma. Squamous cell carcinoma decreased in both
sexes, but more significantly in men. Oat cell carcinoma showed no changes.
The incidence of lung cancer is decreasing for all subtypes in
men, except for adenocarcinoma. The incidence rates in women continue to
increase, particularly for adenocarcinoma. This trend has been observed in the
literature since the current century.11-13 This histological variant is the
most common worldwide, especially in women. This fact could be explained by
several reasons: the increasein the number of female smokers,
the decrease in the overall male smoking population, and changes in smoking
habits, that is to say, the consumpÂtion of filtered and low-nicotine
cigarettes, with consequent changes in the way tobacco smoke is inhaled. On the
other hand, the high percentage of adenocarcinoma among non-smoking women
requires further investigation into the role of other carcinogens apart from
those found in toÂbacco smoke. Several factors are proposed for the development
of this subtype, such as exposure to cooking fumes, environmental pollution, radiaÂtion,
as well as genetic susceptibility, nutritional status, immune dysfunction,
tuberculosis, asthma, and HPV. However, further research is needed to clarify
the main etiology.9
The diagnostic method that yielded the highÂest results in
adenocarcinoma was the CT-guided biopsy, while for squamous cell carcinoma, the
fiberoptic bronchoscopy; this is associated with the anatomical location of
each strain. The evolution of Diagnostic methods throughout these years, from
the sputum cytology until the use of the PET-CAT, EBUS and the availability of
mediastinoscopies have allowed for a more precise diagnosis and the indication
of targeted treatments.14
At the time of diagnosis, 62% of patients were in advanced
non-surgical stages (IIIB and IV), both men and women, as observed in the three
most common histological types analyzed. Even in the second decade, the
increase in stage IV cases was evaluated. This defined the fact that the
primary treatment established was oncological, and contributes to explain the
limited number of potentially curable patients.
Regarding the diagnostic certainty, the percentÂage of patients
who have lung cancer but do not have histological confirmation ranges from 4 to
26% according to different series (11). In our study, there were 65 patients
(13%) with a clinical and radiological diagnosis. Half of these patients were
in stage IV and only received palliative treatment.
As for stage I cases, they represented 12%; and out of the 41
cases, only 16 patients underwent surgery with curative intent. We do not have
data on the follow-up of patients with stages I and II who were operated on in
the first two years to asÂsess recurrence.11,
12
We canât provide information on the improveÂment in adenocarcinoma
survival rates with the new targeted molecular therapies described in the literature due to
the lack of continuity in the follow-up of our patients.
Among
the rare tumors, the carcinoid tumors had the best survival, and all of the
cases underÂwent surgery.
This
study has several limitations, such as data underreporting and lack of patient
follow-up, which prevent us from drawing conclusions.
In
the last decades, we have witnessed a progresÂsive improvement in healthcare in
our country, particularly in the advancements of diagnostic and staging
procedures. Advancements in the staging methods may have shifted the percentage
of patients previously classified as localized stage to non-localized stages.7
However, in our series, we did not observe an increase in patients diagnosed at
regional stages. Emphasizing the importance of early diagnosis to improve
prognosis remains one of the unresolved challenges in the management of lung
cancer patients.
Conflict
of interest
Authors
have no conflicts of interest to declare.
Funding
source
None.
REFERENCES
1.
Consenso Nacional Intersociedades sobre Carcinoma de Pulmón
Células No Pequeñas. Rev Am Med Resp 2019 Mar; Vol 19 (Supl 1):
1-108.
2.
González, M Calvo, V; Barletta, P.; Abriata. M. Boletín
vigilancia epidemiológica: Situación de salud por cáncer
de pulmón y tabaquismo en Argentina. Un aporte para la toma de
decisiones en salud pública basadas en información 2019.
https://bancos.salud.gob.ar/sites/default/files/2020- 03/0000001441cnt-boletin_epidemiologia_situacion_salud_cancer_pulmon_y_tabaquismo_argentina_2019.pdf
3.
Bade BC, De la Cruz CS. Lung Cancer 2020: Epidemiology, Etiology, and
Prevention. Clin Chest Med. 2020;41:1-24.
https://doi.org/10.1016/j.ccm.2019.10.001
4.
McErlean A, Ginsberg MS. Epidemiología del cáncer de
pulmón. Seminarios de Roentgenología. 2011;46:173-7.
5.
Ireri Thirión-Romero, Rogelio Pérez-Padilla, Cecilia
García- Sancho, Luis Torre-Bouscoulet. Tabaquismo y cáncer de
pulmón. Cincuenta años de evidencia. Neumol Cir Tórax.
2018; abril-junio:Vol. 77(No. 2)
6.
Tasas de Incidencia y mortalidad en Cancer en Argentina, The Global Cancer
Observatory, 2020. https://gco.iarc.fr/today/
data/factsheets/populations/32-argentina-fact-sheets.pdf
7.
Arrieta O, Lazcano E. Cáncer de pulmón. El peso de la enÂfermedad
y avances en el diagnóstico y tratamiento. Salud Pública Mex. 2019;61:217-8. https://doi.org/10.21149/10660
8.
Chang JS, Chen LT, Shan YS, et al. Comprehensive Analysis of the Incidence and
Survival Patterns of Lung Cancer by Histologies, Including Rare Subtypes, in
the Era of Molecular Medicine and Targeted Therapy: A Nation- Wide Cancer
Registry-Based Study From Taiwan. MediÂcine (Baltimore). 2015;94:e969. https://doi.org/10.1097/MD.0000000000000969
9.
De Sousa VML, Carvalho L. Heterogeneity in Lung Cancer. Pathobiology. 2018;85:96-107. https://doi.org/10.1159/000487440
10.
Santos-Martínez MJ, Curull V, Blanco ML, y col. CaracterÂísticas
del cáncer de pulmón en un hospital universitario. Cambios
epidemiológicos e histológicos en relación con una serie
histórica. Arch Bronconeumol. 2005 Jun;41:307-12.
https://doi.org/10.1157/13075998
11.
Cilleruelo Ramos A, Figueroa Almánzar S, López Castro R.
Documento de consenso de la Sociedad Española de Cirugía
Torácica. Seguimiento a largo plazo de los pacientes operaÂdos de
cáncer de pulmón. Cirugía Española. 2022;100:320-8. https://doi.org/10.1016/j.ciresp.2021.08.003
12.
Lung Cancer in Adults. Quality standard [QS17]: published March, 26 2012
https://www.nice.org.uk/guidance/qs17
13.
Schneider BJ, Ismaila N, Aerts J, et al. Lung Cancer Surveillance After
Definitive Curative-Intent Therapy: ASCO Guideline. J Clin Oncol. 2020 Mar
1;38(7) https://doi.org/10.1200/JCO.19.02748
14.
Lung Cancer: Diagnosis and Management. NICE guideline [NG122]: published March
28 2019. https://www.nice.org.uk/guidance/ng

| GalerÃa de imÃĄgenes | ||
| Mujer joven con afectaciÃģn pulmonar bilateral y alteraciÃģn de la conciencia | ||
Autores: Churin Lisandro |
 |
|