

Autor : Salcedo Lobera, Esperanza1, Páez Codeso, Francisco M.1, Ruano Carretero, MartĂn A.1
1 Medical-Surgical Clinical Management Unit for Respiratory Diseases. Hospital Regional Universitario de Málaga. Málaga. Spain.
https://doi.org./10.56538/ramr.JQRB8135
Correspondencia : Esperanza Salcedo Lobera. Av. Europa 1, 5º E 29003, Málaga (Spain). E-mail: esalcedolobera@gmail.com
INTRODUCTION
Complete tracheal
rings are the cause of uncommon tracheal stenosis in adult patients, and more
comÂmon in neonates. Only a few cases are reported in the literature, and on
many occasions, adult patients are asymptomatic or show mild respiratory
symptoms similar to other diseases such as asthma. The computed tomography (CT)
is essential to be able to differentiate the structure of tracheal rings and
distinguish it from other diseases, such as stenosis following intubation.
Generally, adult
patients undergo surveillance endoscopy or local treatment, in contrast to
neonates, who receive surgical treatment.
CASE REPORT
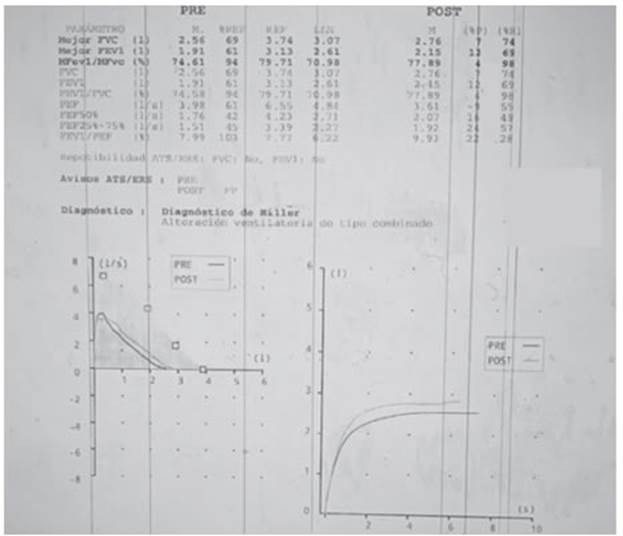
32-year-old woman, no
relevant medical history, referred for dyspnea mMrC (Modified Medical Research
Council Scale) grade II-III/IV 2 years ago. The patient was diagnosed with
asthma through pulmonary functional tests (Figure 1) and allergy skin tests to
pneumoallergens (prick test) positive to mites. During subsequent consultations,
the patient didn’t show any improvement despite the prescribed treatments, such
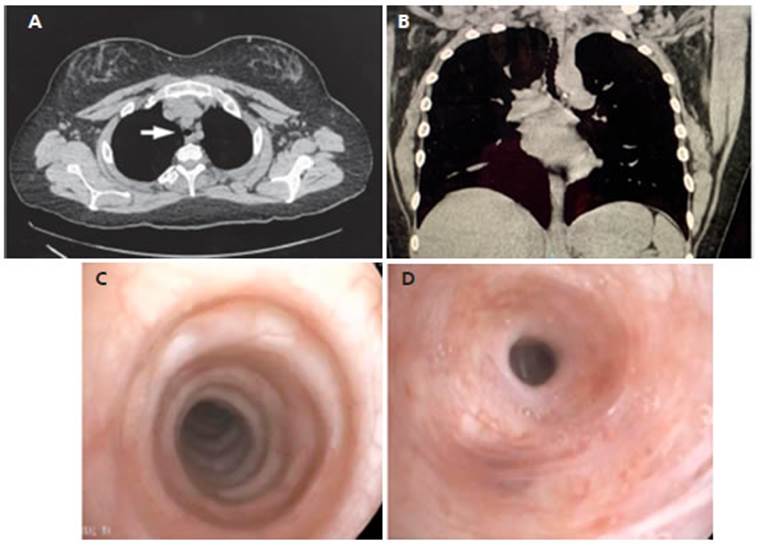
as inhaled bronchodilators, omalizumab and corticosteroids. A CT was performed
to discard any associated disease; it showed globally and uniformly reduced
tracheal caliber (Figures 2 A and B). One bronchoscopy showed complete tracheal
rings throughout the trachea with reduced luÂmen, together with concentric
stenosis of the upper right lobe bronchus, with permeable distal lumen (Figures
2 C and D).
Due to these
findings, the patient was diagnosed with bronchial hyperresponsiveness caused
by heightened sensitivity to pneumoallergens, and she continued receiving
bronchodilators and steroids as needed.
A consensus was
reached on follow-up consultations every six months together with patient
surveilÂlance through spirometry, endoscopy and imaging, taking into account
the patient’s decision, age, and distal permeability of the bronchial tree.
DISCUSSION
Complete tracheal
rings are rare in adult patients; there are very few cases reported in the
literature.1 This condition is
generally diagnosed in neonates, and is characterized by defects occurring
during the embryonic stage in the membranous portion of the tracheal rings,
causing lumen stenosis.
Clinical symptoms are
highly variable. Severe cases are reported in neonates, compared to adult paÂtients,
who are generally asymptomatic or show dyspnea, cough, sibilance or other
non-specific symptoms similar to those of asthma; that is why it should be
included in the differential diagnosis of this disease.1
CT images may be
useful for the diagnosis. These show the narrowing of the tracheal lumen in the
shape of an “O” instead of a “C” appearance, without wall thickening.2
These findings differentiate this condition from other types of
stenosis, such as the one produced after an intubation.
Cases with many
symptoms, which generally occur in neonates, require surgery, even though someÂtimes
the endoscopic follow-up or local treatments (such as tracheal dilation, seen
in adults) are enough.3
Conflict of interests
The authors declare that there is
no conflict of interests.
REFERENCES
1. Nagappan R, Parkin G, Wright CA,
et al. Adult long-segment tracheal stenosis attributable to complete tracheal
rings masÂquerading as asthma. Crit Care Med.
2002;30:238-40. https://doi.org/10.1097/00003246-200201000-00034
2. Boiselle PM, Ernst A, DeCamp MM.
CT diagnosis of complete tracheal rings in an adult. J Thorac
Imaging. 2007;22:169-71. https://doi.org/10.1097/01.rti.0000213563.33044.70
3. Hayasaka T, Kobayashi T, Ako Y,
Endo Y, Saito Y. A case of asymptomatic complete tracheal rings in an adult:
case report. JA Clin Rep. 2019;5:45. https://doi.org/10.1186/s40981-019-0265-7

| GalerĂa de imágenes | ||
| Mujer joven con afectaciĂłn pulmonar bilateral y alteraciĂłn de la conciencia | ||
Autores: Churin Lisandro |
 |
|