

Autor : Larrateguy Luis1, Pais Carlos2,3, Marroni Fabricio3, Riveras Mauricio3, Larrateguy Santiago1
1 Centro Privado de Medicina Respiratoria de Paraná 2 Cardiocom 3Facultad de IngenierÃa. UNER
Correspondencia : ldlarrateguy@gmail.com
Abstract
Chronic respiratory diseases are frequently associated with cardiac autonomic dysfunction and this can be evaluated by measuring post-exercise heart rate recovery (HRR). There is evidence that the HRR calculated after one minute of rest following a Six-Minute Walk Test (6MWT) can predict mortality and acute exacerbations in patients with chronic respiratory diseases.
The purpose of this study is to compare the heart rate recovery after finishing a Three-Minute Step Test (3MST) in chronic respiratory patients with that obtained after the 6MWT.
The 3MST was performed without difficulty in a small doctor’s office and all the patients were able to finish it. Applying the Pearson Correlation Index, the result was 0.84 when comparing the HRR one minute after stopping in both tests, showing a good correlation between them.
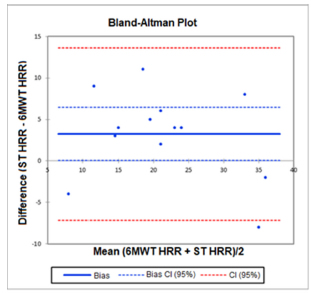
In the Bland-Altman Plot, we can see that the results are within the confidence limits and show concordance despite being a small sample of patients.
The 3MST is easily done in a small doctor’s office. The results of the HRR after the 3MST are comparable to those obtained after finishing the 6MWT.
Key words: Heart rate control; Exercise test; Step test.
Introduction
Post-exercise heart rate recovery is a marker of cardiac autonomic dysfunction and in some chronic diseases its reduction is related to a bad prognosis1-4.
Chronic respiratory diseases are associated with cardiac autonomic dysfunction, and it has been proven that the HRR, calculated after one minute of rest using the 6MWT is important to predict mortality in patients with chronic respiratory diseases1-3. It has been recently reported that a HRR of less than 14 beats post-6MWT is an independent predictor of acute exacerbations in patients with COPD (chronic obstructive pulmonary disease)4.
However, Tramontini et al observed that there are variations in the 6MWT, in terms of methodology, the place where it is performed, the distance of the hall that is used, the number of tests performed and the way in which patients are motivated during the tests (words of encouragement, time intervals and supervisor position). All of this reduces reliability and makes it impossible to compare results5. On the other hand, both the 6MWT and the step tests, regulated by time, have the characteristics of a submaximal test, that is why in Brazil the step test has been suggested to evaluate exercise tolerance in healthy patients and patients with COPD6.
The purpose of this study is to measure the HRR one minute after finishing a step test set with a fixed step-up cadence and a duration of three minutes (3MST) in patients with chronic respiratory disease and compare it with the HRR obtained after a 6MWT evaluating the feasibility of performing the 3MST in a doctor’ office.
Materials and Methods
We evaluated 13 patients with chronic respiratory diseases at the Centro Privado de Medicina Respiratoria de Paraná. All of them performed the 6MWT and the 3MST the following day in the same time period between 5 and 7 p.m.
The following were considered as inclusion and exclusion criteria: having a chronic respiratory disease, being clinically stable, without symptomatic cardiovascular disease or treatment with beta blockers, without any neurologic disease or any other condition that could affect the capacity to perform a submaximal exercise test.
The 6MWT was performed in accordance with the rules of the ATS/ERS (American Thoracic Society/ European Respiratory Society)7, using a Nellcor Puritan Bennet NPB-40® oximeter after the six-minute walk and then one minute after that, with the patient seated and at rest.
The 3MST was performed in an office of the Centro Privado de Medicina Respiratoria de Paraná. It consisted in going up and down a 20 cm-high step that was built ad-hoc with a cadence of 20 step-ups per minute indicated by a metronome every three minutes. The equipment used was designed by Cardiocom, and consisted of a pulse oximeter with an algorithm calculating the HRR after finishing the three-minute exercise and one minute after that, with the patient seated and at rest.
Results
To compare the HRR of the 3MST and the HRR of the 6MWT we used the Pearson Correlation Index (CI) and obtained 0.84 as a result, showing good correlation between both tests.
In the Bland-Altman Plot, we can see that the results are within the confidence limits and show concordance despite being a small sample of patients.
Discussion
The three-minute step test with measurement of the HRR and the device to measure it are easy to use inside a small doctor’s office.
The 6MWT is at present the most widely used test to estimate exercise tolerance in patients with respiratory diseases. But, in daily medical practice, it is difficult to meet the standards of the American Thoracic Society (ATS) and the European Respiratory Society (ERS)7, since the main purpose of the 6MWT is to measure the distance traveled by the patient during a 6 minute walk on a flat, leveled, obstacle-free floor between 15 and 30 meters long, possibly round and without other people walking around. It is hard to meet all of those requirements at the office, thus making it difficult to compare results obtained in different health centers, mainly in research studies5.
On the other hand, the step test is an exercise test with the advantages of being simple, portable and with the possibility to be done in a reduced space. At present, this test is not widely used to evaluate patients with respiratory diseases, but tests have been done in patients with asthma, cystic fibrosis, idiopathic pulmonary fibrosis, stroke and COPD8-10. This test is not standardized and there are various protocols applicable both to healthy and ill patients. Standardization differences lie in the height of the step, the speed in which the patient has to go up and down the step (cadence) and the duration of the test.
When deciding about the height of the step, we took into account the fact that there are tests that used 20 cm-high steps that older people could carry out without any difficulty11 and on the other hand, this height is usually used in Argentina for the steps of staircases in houses and buildings.
The step tests used in healthy subjects or patients with respiratory diseases can be done with free or regulated cadence12, 13.
Fixed-cadence step tests are useful for comparing cardiopulmonary responses under similar workloads. If the heart rate is maintained between aerobic levels, it is a submaximal test (the same intensity as the 6MWT), therefore it is safe. This is not possible in tests with free cadence, that is to say, at a rhythm fixed by the patient himself, since the variability in the number of step-ups modifies the work done by the patients6.
In a study conducted in Quebec only 49 of the subjects completed the 32-step test, but most patients were able to complete the test with a cadence of 18 and 26 steps23. In another study, this group observed that 90 and 85% of the subjects were able to complete the test with the cadence of 16 and 20 steps, respectively8.
The duration of the test also varies greatly according to the protocols used so far6, 8, 9.
Some have certain degree of incremental physical demand, increasing cadence at an externally established rhythm, and ending the moment symptoms appear6; in other tests, instead, the patient is asked to go up the step 15 times as fast as he can13; and there are other tests with a fixed total duration that varies from 90 seconds to 10 minutes9, 10.
The suggested protocol in this study establishes a fixed duration of 3 minutes with the purpose of achieving, together with the step height (20 cm) and set cadence (20 steps per minute), a physical demand level that is representative of a submaximal exercise test.
The patients didn’t have difficulty in doing the step test, which was shown to be
easily performed in a small office. There weren’t any problems, either, with the set cadence or step height. But, one patient felt pain in the hip and another one said his lower limbs felt tired. Both patients completed the test.
HRR is a reflex of the reduced vagal activity and a powerful predictor of global mortality regardless of the workload, the presence or lack of myocardial perfusion and changes in heart rate during
exercise14, 15. In this study, the HRR obtained with the suggested 3MST is comparable with that obtained with the 6MWT.
Although results are encouraging, the number of individuals studied in this sample is small. With a larger sample of patients we would be able to evaluate the reproducibility of this test and the clinical usefulness of the HRR obtained from the exercise tolerance evaluation as a predictor of mortality and from the evaluation of the pharmacological and non-pharmacological treatment in patients with respiratory diseases.
Conflicts of interest: None
1. Lacasse M, Maltais F, Poiri P, Marquis K, Jobin J, LeBlanc P. Post-exercise heart rate recovery and mortality in chronic obstructive pulmonary. Respiratory Medicine. 2005; 99: 877-86.
2. Swigris JJ, Swick J, Wamboldt FS, et al. Heart rate recovery after 6-min walk test predicts survival in patients with idiopathic pulmonary fibrosis. Chest. 2009; 136: 841-8.
3. Gupta M, Bansal V, Chhabra SK. Abnormal heart rate recovery and chronotropic incompetence on exercise in chronic obstructive pulmonary disease. Chron Respir Dis. 2013; 10: 117-26.
4. Rodríguez DA, Kortianou EA, Alison JA, et al. Heart Rate Recovery After 6-min Walking Test Predicts Acute Exacerbation in COPD. Lung. 2017: 195: 463-7.
5. Tramontini MR, Mayer AF, Cardosoa F, et al. Variabilidad en las condiciones de la prueba de la marcha realizada en el contexto de programas de rehabilitación pulmonar en América Latina y en la Península Ibérica. Arch Bronconeumonol. 2005; 12: 667-78.
6. Andrade CH, Cianci RG, Malaguti C, et al. The use of step tests for the assessment of exercise capacity in healthy subjects and in patients with chronic lung disease. J Bras Pneumol. 2012; 38: 116-24.
7. Holland AE, Spruit MA, Troosters T, et al. An official European Respiratory Society/American Thoracic Society technical standard: field walking tests in chronic respiratory disease. Eur Respir J 2014; 44: 1428-46.
8. Borel B, Wilkinson-Maitland CA, Hamilton A, et al. Three-minute constant rate step test for detecting exertional dyspnea relief after bronchodilation in COPD. Int J Chron Obstruct Pulmon Dis. 2016; 11: 2991-3000.
9. Da Silva T, Raimundo RD, Ferreira C, et al. Comparison between the six-minute walk test and the six-minute step test in post stroke patients. International Archives of Medicine, 2013; 6: 31.
10. de Camargo AA, Justino T, de Andrad CH, et al. Chester step test in patients with COPD: reliability and correlation with pulmonary function test results. Respiratory Care. 2011; 56: 995-1001.
11. Cho B, Scarpace D, Alexander N. Tests of Stepping as Indicators of Mobility, Balance, and Fall Risk in Balance-Impaired Older Adults. J Am Geriatr Soc. 2004; 52: 1168-73.
12. Young RP, Holst PE. A simple exercise test in assessment of asthma. N Z Med J. 1988; 101: 600-1.
13. Jones P, Wakefield J, Kontaki E. A simple and portable paced step test for reproducible measurements of ventilation and oxygen consumption. Thorax. 1987; 42: 136-43.
14. Cole C, Blackstone E, Pashkow F, et al. Heart-rate recovery immediately after exercise as a predictor of mortality. N Engl J Med. 1999; 341: 135-7.
15. Starobin D, Kramer MR, Yarmolovsky, et al. Assessment of functional capacity in patients with chronic obstructive pulmonary disease: correlation between cardiopulmonary exercise, 6-minute walk and 15 step exercise oximetry test. Isr Med Assoc J. 2006; 8: 460-3.
06; 8: 460-3.

| GalerÃa de imágenes | ||
| Mujer joven con afectación pulmonar bilateral y alteración de la conciencia | ||
Autores: Churin Lisandro |
 |
|