

Autor : Luis Javier Nannini1 *
1Hospital “Eva Perón”. G Baigorria. Pulmonology Faculty of Medical Sciences, Universidad Nacional Rosario. Argentina
Correspondencia :Luis Javier Nannini - E-mail: ljnannini@hotmail.com
Abstract
Introduction:
Global asthma mortality is still an unresolved issue, despite the
existence of highly effective treatments. This occurs in Argentina, where there
are also some effective treatments, but there is few
information about the relationship between asthma mortality and sales of
inhaled medication. The purpose of this study was to analyze sales in
pharmacies of medication for obstructive respiratory diseases and asthma
deaths, before and after the appearance of inhaled corticosteroids (ICSs) and
their combinations.
Materials and Methods:
An official bulletin was the source document for data about asthma
mortality in Argentina between 1983 and 2018. All data on pharmacy sales were
provided by the same source (IQVIA Solutions Argentina), but there are no sales
data from 1990 to 1999.
Results:
The mean ± standard deviation of the ratio between total sales of short-acting β
2-adrenergic agonist bronchodilators (SABAs) over total sales of ICS and
their combinations was 13.68 ± 2.85 between 1983-1988 and 1.03 ± 0.12 between
2010-2019 (p < 0.0001). There was a significant correlation between the
SABA/ICS ratios and the number of asthma deaths from 1983 to 2018 (Pearson
correlaÂtion: r = 0.977, p < 0.0001). During the period from 2010 to 2018
there was a significant decrease in the number of deaths compared to 1980-1989
(145.9 ± 28.58 vs. 43.1 ± 5.2; p <0.0001). Since 2016, SABA sales started to
decrease and were overtaken in 2019 by the combinations of ICS/long-acting
b2-agonist bronchodilators (LABAs).
Conclusions:
The significant correlation between the SABA/ICS sales ratio and asthma
deaths would make us rethink the long-established treatment stereotype of SABAs
for the management of asthma.
Key words:
Sales of medication; Mortality,
Asthma; Argentina
Received: 09/07/2020
Accepted: 04/08/2021
SABA - short-acting β
2-agonist bronchodilator
ICS - inhaled corticosteroid
LABA - long-acting β
2-agonist bronchodilator
LAMA - long-acting
muscarinic antagonist
ICD - International
Classification of Diseases
GDP - Gross
Domestic Product
COPD - chronic obstructive
pulmonary disease
Introduction
The marketing department of
pharmaceutical industry is usually in charge of the information regarding the
sales of drugs. This information is very expensive and used for purposes other than
epidemiology and public health. Also, mortality rates are studied by
epidemiologists and public health physicians who have no access to the sales of
drugs. Only on rare occasions the sales of drugs and mortality rates are
analyzed jointly. The epidemic outbreaks that caused asthma deaths associated
with isoproterenol in the United Kingdom and fenoterol
in New Zealand are clear examples of the importance of analyzing the mortality
and drug sales variables jointly1.
The increased knowledge of asthma inflammation and the availability of inhaled corticosteroids produced an important decrease in the global asthma mortality rate since the 1990s2-5. Despite these achievements in the treatment of asthma, global asthma mortality has been stalled since 20061, 2, 4. Short-acting β
2-adrenergic agonist bronchodilators (SABAs) are still a deeply rooted
stereotype of the asthma treatment on a global scale, regardless of the
positive correlation between SABA use and the increase in asthma mortality3. In the case of
salbutamol, the initial scientific evidence was only a 300-minutes study
carried out in 24 patients to observe the bronchodilating
action6. The SABAs do
not have an anti-inflammatory action, and subjects with asthma may develop
overreliance on SABA, thus promoting the withdrawal of the controller
medication7.
The purpose of this study was to
analyze sales in pharmacies of medication for obstructive respiraÂtory diseases
and asthma deaths, before and after the appearance of inhaled corticosteroids
(ICSs) and their combinations.
Materials and Methods
Since the beginning of 2020 we began to gather data for this descriptive, retrospective study. We started to analyze the trend of sales in pharmacies of medication for obstructive respiratory diseases and on the other hand the deaths from asthma. Two different periods of time were taken into account. The first stage, between 1983 and 1989, where effective ICSs weren’t still available (there were low doses of beclomethasone and disodium cromoglycate), and the other stage between 2000 and 2019, with opÂtimum doses of ICSs and ICSs in combination with long-acting β
2-agonist bronchodilators (LABAs).
Mortality data in Argentina were
collected from an official report published by the Instituto
NacioÂnal de Enfermedades Respiratorias “Emilio Coni” (National
Institute of Respiratory Diseases “Emilio Coni”) and
the National Administration of Laboratories and Health Institutions, Ministry
of Health (Argentine Republic)8.
This report about asthma mortality shows the absolute values between 1980 and
2018 and the crude and age-adjusted asthma mortality rate curves per 100,000
inhabitants in ArÂgentina within the 5-39 age group (ICD 9: 493 and ICD 10:
J45-J46)8. The official
site for the national asthma mortality data has been unavailable since October
2020.
The source of data about the
sales in pharmacies of drugs for obstructive respiratory diseases in ArÂgentina
was the same for both periods. The data used from 1983 to 1990 had been already
published by IQVIA Solutions Argentina (former IMS HealthInc),
available in Table 1 of the Molfino et al article9, and from 2000 to 2019,
unpublished data were used, obtained by courtesy of IQVIA. There are no sales
records between 1990 and 1999.
In order to obtain the SABA/ICS
ratio, all the short-acting inhaled bronchodilators of every year were added
and then divided by the sales of beclomethasone for
the 1983-1988 period. From 2000 to 2019, the sales of
short-acting inhaled bronchodilators were added year after year, and the
denominator of the SABA/ICS ratio was the sum of all the ICSs used for monotherapy plus all the ICS/LABA combinaÂtions (Table 1).
Oral theophylline and montelukast were considered
separately.
Results are shown as mean ±
standard deviation (SD). In order to analyze if two variables are related
(SABA/ICS sales ratio and asthma deaths), we applied the Pearson correlation
coefficient as a measure of linear dependence between two quantitative
variables. The result of the analysis is a correlation coefÂficient with values
between -1 and +1. The Independent Sample Student T Test was used to evaluate
if there was a significant difference between the mean number of deaths and the
SABA/ICS ratios in the two groups (both decades), after checking if there was
normal distribution with the F test. A p-value < 0.05 was considered
significant. We used the Instat-Graphpad program.
Results
Table 1 shows
annual sales of SABAs and ICS/LABA, the ratios between both and finally asthma
deaths in individuals between 5 and 39 years. The mean SABA/ICS sales ratio
between 1983 and 1988 was 13.68 ± 2.85 (mean±SD).
This means that for every sold unit of ICSs, 13.68 units of SABAs were sold
(see Table 1). The SABA/ICS sales ratio of the period 2010-2019 was 1.03
± 0.12, significantly lower than the 1983-1988 ratio
(p < 0.0001; Table 1).
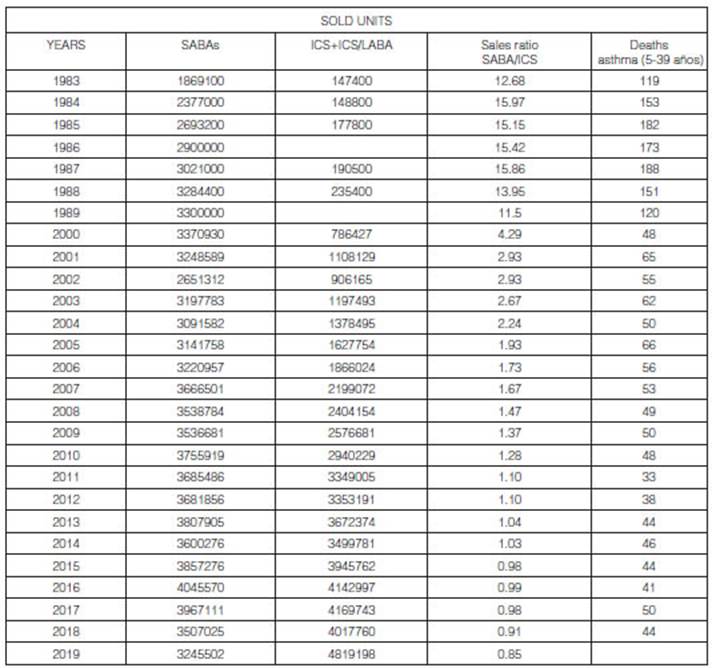
SABA: units of inhaled bronchodilators sold in pharmacies in Argentina.
ICS+ICS/LABA: sales in units of inhaled corticosteroids plus combinations of
corticosteroids and long-acting bronchodilators. SABA/ICS ratio: result of the
division between the total sales of SABAs/total sales of ICSs+ICSs/
LABAs. Asthma deaths reported by the “Emilio Coni” Institute within the 5-39 years age group.
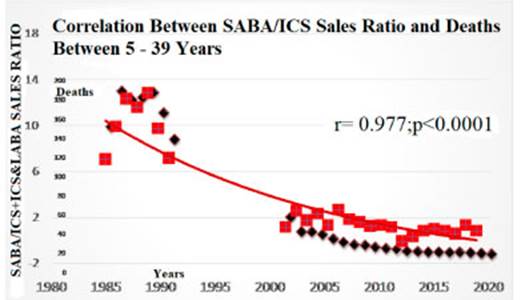
Correlation between asthma deaths and the SABA/ ICS ratio: r = 0.977; p <
0.0001 according to the Pearson Correlation Test. The mean values of the
SABA/ICS sales ratios between 1983 and 1988 were 13.68 ± 2.85 (mean ± SD)
versus the 2010-2019 period (1.03 ± 0.12; unpaired T Test: p < 0.0001).
A correlation was found between the SABA/ICS sales ratio and the number of asthma deaths (r = 0.97; p < 0.0001) according to the Pearson Correlation
Figure 1. Deaths from asthma
showed a significant decrease in the 5-39 age group, when average deaths from
the 1980-1989 decade were compared to those of the 2020-2018 period (mean 145.9
± 28.58 vs. 43.1 ± 5.2; unpaired T Test; p < 0.0001).
Discussion
The most important finding of
this study was to show for the first time in Argentina, a correlation between
the SABA/ICS sales ratio and asthma deaths so that the lower the ratio (because
the ICS sales ratio is higher) the lower the number of deaths. A greater number
of ICS sales would suggest that the inflammatory aspect of asthma is being
treated without distractions as with bronchodilators. EnÂcouraging the
treatment of the inflammation should be the keystone of every health policy on
asthma.
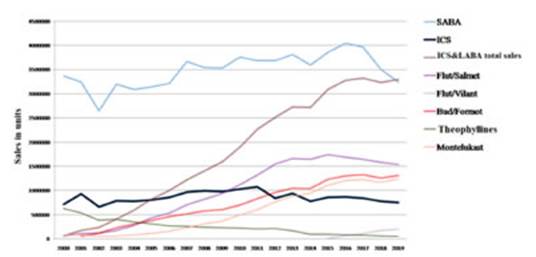
In 2019, the sum of all ICS/LABA combinations without the ICSs used for monotherapy was able to surpass the sales of SABAs, for the first time in history Figure 2).
Due to the appearance of the SARS-CoV2 pandemic, it will be very
difficult to analyze data from year 2020. The first ICSs was
beÂclomethasone, which reached peak sales in 1987
with 165,000 units, even though it represented less than 2% of the total sales
of that year9.
The concentration of beclomethasone was 50 μg as metered-dose
inhaler and the minimum anti-inflammatory dose is 400 μg/day. An individual
had to inhale 8 daily doses. Between 2010 and 2019, the ICSs plus their
combinations always sold over 3 million units. The SABA/ICS sales ratio started
to decrease at the end of the 1980s (not taking into account the sales of oral
bronchodilators); but since 2010, the constant increase in the sales of ICSs
and their combinations achieved a SABA/ICS ratio close to one. Such decrease in
the ratio was produced only by an increase in the denominator until 2016; since
that year the numerator (SABA sales) began a slow decrease together with the
continuous increase in the denominator (ICS sales). As the ratio decreased,
asthma deaths started to decline8 (see Figure 1) and both
variables (ratio and deaths) showed a significant corÂrelation from 1983 to
2018 (Pearson correlation, r = 0.97; p < 0.0001). Beyond the objections to
death certificates10;
by excluding individuals under 5 years old, deaths from bronchiolitis are not
counted, and by excluding individuals older than 39 years, COPD deaths are
discarded. Thus, the 5-39 age group provides more
accuracy to the data obtained from death certificates.
With the arrival of very
effective ICSs and the promotion activities performed by some organizations
such as GINA11 a deceleration in the asthma
mortality rate in Argentina could be achieved12.
This ausÂpicious phenomenon occurred on a global level; but reached a plateau
in 2006 that is still sustained2.
The high consumption of SABAs between 1983 and 1989 could be related to deaths
from asthma, as has happened in other countries1.
We can’t say that the high consumption of SABAs over mortality is a matter of
causality, nevertheless, the correlation found between the SABA/ICS sales ratio
and the deaths (r = 0.97; p < 0.0001) supports the hypothesis of a
relationship. This correlation emphasizes the need to insist on treating
inflammation.
In order to place the Argentinian
situation within the world context, we can observe the Finland phenomenon,
where a successful 10-year program was implemented from 1994 to 2004 based on
the anti-inflammatory intervention from the outset13.
In 1987, one third of asthma patients in Finland were under treatment with ICSs
(in Argentina less than 2% of sales) and in 2004 more than 85% of patients who
purchased medication for asthma at the pharmacy were using ICSs on a daily
basis13. In 2005
Finland achieved a ratio of 1 of daily doses of ICS/SABA and during the period
from 1990 to 2003 there were only 10 deaths from asthma in individuals under
20. However, with the Finnish program, 72% of patients were using SABAs almost
every day, 35% used a course of oral corticosteroids, there were 18% of asthma
hospitalizations and to its advantage, asthma deaths of patients of all ages
decreased from 123 to 85 seven years after the program had begun14.
The SABAs were part of the program because there weren’t any alternatives. Not
eradicating the SABAs from the program may have influenced the fact that the
results weren’t more categorical.
With a much different data
processing, this study shows that it was only in 2015 that Argentina took the
SABA/ICS consumption ratio to 1; but Finland calculated the ratio in doses, and
in Argentina it was calculated per units sold, where one unit may contain
between 200 and 250 doses and between 30 and 200 ICS and their combinations.
This would mean that treatments with ICSs wouldn’t be available for most of the
asthmatic population in Argentina.
Since 2015 the sales growth of ICSs used as monotherapy has stalled, but ICS/LABA combinations began to increase. The use of SABAs started to decrease in 2016 (Figure 2
). Since 2015, the SABA/ICS ratio has remained under 1. This doesn’t
imply that the SABA hegemony was over in 2015; but the descending trend has
been maintained for 4 uninterrupted years and for the first time the SABAs were
surpassed by another drug category in 2019. We will have to wait a few years to
know if that trend is consolidated.
If we analyze the sales of
fluticasone/salmeterol separately (Figure 2), we can observe that with 12 commercial brands a very mild decrease
has started since 2016. The ICSs used as monotherapy
showed a similar trend with 28 commercial brands. On the other hand, an
ascending trend can be observed since 2014 with budenoside/formoterol (with 8 brands), montelukast
(14 commercial brands) and flutixcasone/vilanterol, which appeared in 2015.
Most asthmatic patients use
controller and rescue medication but are unaware of the advantages of
controller medications15 and loose adherence, because
they rely on the immediate bronchodilating effect of
the SABAs7. Budesonide/formoterol is the exception because it can also be used as
rescue agent16.
In this regard we could say that the decrease in the sales of SABAs, ICSs and
fluticasone/salmeterol could be explained by the growing
use of the anti-inflammatory rescue strategy with budenoside/formoterol that substitutes both the SABAs and other
controller drugs. Every patient using SABAs could develop an overreliance that
could increment the risk of death and asthma attacks with life-threatening risk3,7.
This overreliance and the increasing use of SABAs was the strongest
characteristic both in patients who died from asthma7,10
and in patients with life-threatening attacks7,
17. We published a document with inÂformation about these
SABA-related risks18 in order to warn the
scientific community in Latin America.
Monotherapy
with LABAs for asthma is prohibited by all the regulatory entities and
international recommendations16 for much less evidence against
them than the SABAs. Monotherapy with SABAs should
have the same recommendation. Additionally, the essential study of salbutamol
with 24 patients lasted 5 hours6,
and any regulatory entity would approve it at present for chronic asthma.
Evidence regarding the deleterious effect on asthma7,
and more importantly the dose-response relationship in mortality3
justify the warning about the use of SABAs in asthma18.
The 2018-2019 negative trends for
SABAs, ICSs and fluticasone/salmeterol could be
related to the decline in Argentina’s GDP19;
but budesonide/formoterol, fluticasone/vilanterol and montelukast conÂtinued
rising and their prices are much higher than those of the SABAs. Also, the
total sales are not related to the natural growth of the Argentinian population
that has been dropping since 1960, though it has always been positive. In the
1980-1991 census, the average annual growth rate was 14.7 per thousand (1.47%);
in the 1991-2001 decade, 10.1 per thousand (1.01%); and between 2001 and 2010,
11.4 per thousand (1.14%)20.
Among the limitations of this
study, there is the fact of not being able to identify the recipients of the
sales, since there are many indications to prescribe the SABAs, such as COPD,
respiratory infections and other obstructive diseases besides asthma. Given
that it is not possible to effectively know if the asthmatic population
in Argentina are the recipients of such sales, we could refute the
relationship between the high asthma mortality in Argentina during the eighties
and the large amount of SABA sales. However, epidemiological studies of large
databases such as Canada found a relationship between risk of death from asthma
and SABA consumption because, among other important aspects, they could
evaluate asthma-only prescriptions3.
The other limitation of this
study is the fact that sales correspond to pharmacies and don’t include
purchases made by official entities for public health plans of free
distribution, hospital purchases and direct purchases, such as biological
therapies.
To conclude, asthma mortality in
Argentina for the 5-39 age group continues to plateau
and, on the other hand, the SABAs were top-selling medications for obstructive
respiratory diseases until 2018. Finding a significant correlation between the
SABA/ICS sales ratio and deaths from asthma should warn the authorities and the
scientific community. If the descending trend in SABA sales is sustained with
an increase in the ICS or ICS/LABA sales, the asthma mortality rate plateau
could finally break in a few years.
Declaration of conflicts of
interest not related to this draft: Collection
of fees as speaker for AstraZeneca and Sanofi-Genzyme.
 References
1. Crane J, Pearce N, Burgess C, Beasley R. Asthma
and the β agonist debate. Thorax 1995; 50 (suppl 1): S5-10
2. Ebmeier SJ, Thayabaran D, Braithwaite I, Benamara
C, Weatherall M, Beasley R. Trends in international
asthma mortality: analysis of data from the WHO Mortality Database from 46
countries (1993-2012). Lancet 2017; 390: 935-45.
3. Suissa S, Ernst P, Boivin JF, et al. A cohort analysis of excess mortality in
asthma and the use of inhaled beta-agonists. Am. J. Respir.
Crit. Care Med. 1994; 149: 604-10.
4. Forno E, Gogna M, Cepeda A, et al. Asthma
in Latin America. Thorax.
2015; 70(9):898-905. doi: 10.1136/thoraxjnl-2015-207199.
5. The Global Asthma Report 2018. Auckland, New
Zealand: Global Asthma Network, 2018. www.globalasthmanetwork.org.
6. Choo-Kang YFJ, Simpson
WT, Grant IWB. Controlled comparison of the bronchodilator effects of three
B-adrenergic stimulant drugs administered by inhalation to patients with asthma.
Br Med J 1969;2: 287.
7. Nannini LJ. Overreliance link between asthmatic subjects and short-acting β2 agonists. Pulm Pharm Ther. June 2018; 50: 80-1.
>8. Instituto Nacional de Enfermedades Respiratorias (INER) “Dr. Emilio Coni”. Administración Nacional de Laboratorios e Institutos de Salud (ANLIS)
“Dr. Carlos G Malbrán”. BoletĂn Mortalidad por asma
de 5 a 39 años en Argentina de 1980 a 2016. http://www.anlis.gov.ar/iner/wp-content/uploads/2020/02/PanelAsmaArgentina-1.html.
Ăšltimo ingreso, abril 2020.
9. Molfino NA, Nannini LJ, Chapman K, Slutsky A.
Trends in Pharmacotherapy for chronic airflow limitation in Argentina: 1983-90.
Medicina (Buenos Aires) 1994; 54:
103-9.
>10. Nannini  (h) LJ. Mortalidad asociada al asma en el Municipio de
Rosario. Medicina (Bs As) 1995; 55: 647-51.
11. Masoli M, Fabian D,
Holt S, Beasley R, Global Initiative for Asthma (GINA) Program. The global
burden of asthma: Executive summary of the GINA Dissemination Commitee report. Allergy. 2004; 59: 469-78.
12. Neffen H, Baena-Cagnani C, Passalaqua G, Canonica GW, Rocco D. Asthma mortality, inhaled steroids
and changing asthma therapy in Argentina (1990-1999). Respir>Med. 2006; 100: 1431-5.
>13. Haahtela T, Tuomisto
LE, Pietinalho A, et al. A 10 year asthma programme
in Finland: major change for the better. Thorax. 2006;61: 663-70.
14. Kauppi P, Peura S, Salimäki J, Järvenpää S, Linna M, Haahtela T . Reduced severity and improved control of
self-reported asthma in Finland during 2001-2010. Asia Pac Allergy 2015; 5: 32-9.
15. Nannini LJ, Neumayer NS, Fernandez OM, Flores DM. Out- patient Asthma
Management without Rescue Bronchodilators? J Pulm Med Respir Res 2019; 5: 024.
16. GINA Executive Committee. Global Strategy for Asthma
Management and Prevention, Global Initiative for Asthma (GINA) 2019. www.ginasthma.org
[18 marzo 2020].
17. Nannini  (h) LJ. Asma potencialmente fatal. Arch. BronconeumologĂa.
1997; 33: 462-71.
18. Nannini LJ, Luhning S, Rojas RA, et al. Position Statement: Asthma in
Latin America. Is Short-Acting Beta-2 Agonist Helping or Compromising Asthma
Management? J Asthma. 2020 https://doi.org/10.1080/02770903.2020.1777563
19. https://datos.bancomundial.org/indicador/NY.GDP.MKTP.KD.ZG?locations=AR. Ăšltimo ingreso en Marzo 2020.
20. Censo Nacional de PoblaciĂłn, Hogares y Viviendas
2010 Censo del Bicentenario Resultados definitivos, Serie B N° 2. p. 62.

| GalerĂa de imágenes | ||
| Mujer joven con afectaciĂłn pulmonar bilateral y alteraciĂłn de la conciencia | ||
Autores: Churin Lisandro |
 |
|