

Autor Gallego Claudio1, Amiano NicolĂ¡s2, Armitano Rita1, Joza Karla1, Tateosian Nancy2, Muñoz Luis1, Poropat Alejandra1, Stupka Juan1, Salomone CĂ©sar1, GarcĂa VerĂ³nica2
1 Hospital General de Agudos Parmenio Piñero, Autonomous City of Buenos Aires, Argentina
2 Faculty of Exact and Natural Sciences, UBA (University of Buenos Aires) - CONICET (National Scientific and Technical Research Council), Autonomous City of Buenos Aires, Argentina
Correspondencia : Claudio Gallego - Av. Varela 1301 (CABA) - ZC 1406 - e-mail: cgallego@intramed.net
Abstract
The epidemiological control strategy of tuberculosis (TB) includes both the diagnosis and early treatment of baciliferous patients and the identification of individuals with latent tuberculosis infection (LTBI), who represent the pathogen reservoir within the population.
Objective: To compare the results obtained using the tuberculin test (PPD, Purified Protein Derivative) and the QuantiFERON-TB Gold Plus (QTF) in a group of household contacts of patients with bacillary pulmonary TB in the city of Buenos Aires. We used two cutoff points to consider PPD as positive: ≥ 5 mm (PPD-5) and ≥ 10 mm (PPD-10).
Materials and Methods: Blood samples for QTF were taken from household contacts of patients with bacillary TB, followed immediately by the application of PPD. The QTF was considered as the reference test from which to compare the PPD by calculating sensitivity (S), specificity (E), positive predictive value (PPV), negative predictive value (NPV) and Kappa correlation coefficient.
Results: 48 contacts were included (33 women, 69%), age 38.8 ± 19 years, 27 (56%) Argentinean, 18 (38%) Bolivians and 3 (6%) Peruvians, 37 were cases of TB. Only one contact informed She/she hadn’t received the BCG; and 44 subjects showed the BCG scar. The QTF was positive in 23 individuals (47.9%) and undetermined in 2 cases (4.2%). Excluding the indeterminate cases from the analysis, there were no significant differences between positive and negative QTF contacts regarding age (33.8 ± 16 vs. 42.1 ± 20 years), nationality: Argentinean (12 of 26.46%) vs. foreigners (11 of 20.55%) and sex: women (18 of 32, 56%) vs. men (5 of 14, 36%).
There were 28 (60.9%) positive cases with PPD-5 and 13 (28.3%) with PPD-10. Comparison between PPD-5 vs. PPD-10: S = 73.9 vs. 34.8%, E = 52.2 vs. 78.3%, PPV = 60.1 vs. 61.5% and NPV = 66.7 vs. 54.5%. The coincident results (positive and negative) between QTF and PPD were 29 (63%) for PPD-5 and 26 (56.5%) for PPD-10. Expressed with the Kappa coefficient, they show weak (0.261) and insignificant (0.130) concordance, respectively.
Conclusions: Considering the QTF as the reference method for its higher specificity, PPD-5, although less specific, was more sensitive than PPD-10 for the diagnosis of latent tuberculosis infection in the group of household contacts under study.
Key words: Tuberculosis; Latent tuberculosis; Tuberculin test; Interferon-γ test; Quantiferon.
Introduction
The epidemiological control strategy of tuberculosis (TB) includes both the early diagnosis and treatment of baciliferous patients and the identification of individuals with latent tuberculosis infection (LTBI). The latter represent the bacillary reservoir in the population, and although most of them will remain asymptomatic, we estimate that 10% of them will develop the disease: generally within two years after the contagion, perpetuating the infectious cycle1.
There isn’t any test to effectively diagnose the presence of LTBI or distinguish which of the infected patients will develop the disease.
Historically, the Tuberculin Test (TT) is used basing on the detection of the late sensitivity immune response to antigens of tuberculous mycobacteria from a Purified Protein Derivative (PPD). This test is limited by the fact that it shows cross-reactions with non-tuberculous mycobacteria and with the BCG (Bacillus Calmette-Guérin) (in Argentina, it is applied to newborn babies).
In recent years, an alternative test began to be used: the measurement of interferon-γ released by sensitized lymphocytes (Interferon-Gamma Release Assay, IGRA) exposed to TB antigens. Among these tests, the QuantiFERON-TB Gold Plus (QTF) exposes lymphocytes to antigens ESAT-6 and CFP-10, which are specific for Mycobacterium tuberculosis, and the results are not influenced by the BCG and don’t show cross-reactions with most atypical mycobacteria (except for Mycobacterium kansasii, szulgai and microti)2.
Since most studies about LTBI indicate higher specificity of the QTF in comparison with the tuberculin test3, in this work we proposed the evaluation of the sensitivity and specificity of the PPD considering the QTF as the reference test, using two PPD cutoff points (5 and 10 mm) in a group of household contacts of patients with bacillary pulmonary TB.
Materials and Methods
The study included household contacts (teenagers and adults) of patients with bacillary TB treated in our Center. We define the household contact as the person living in the same house as the patient (> 6 hours/day) for at least three months before the TB diagnosis. The inclusion of contacts was limited to a maximum of two per index case.
All of the contacts underwent a clinical evaluation and chest x-ray (CxR), and the BCG vaccine application was recorded (skin scar). Subjects with positive serologic test for HIV or another immunosuppression cause, history of TB, finding of TB in the CxR (active or residual) or with history of positive PPD or its application in the last 10 years4 were excluded from the study.
After signing the informed consent, blood was extracted for the QTF (QuantiFERON-TB Gold Plus, QUIAGEN, Germany), and hemogram and serologic tests were conducted for HIV, followed immediately by the application of PPD by means of the tuberculin test. We used PPD LM-08 tuberculin (Malbrán Institute, Argentina), applied and read by trained personnel.
Results obtained about sensitivity (S), specificity (E) and positive and negative predictive values (PPV, NPV) were compared for the cutoff points of PPD ≥ 5mm (PPD-5) and ≥ 10mm (PPD-10) using the QTF as reference method, and the agreement between tests by kappa coefficient was assessed. Data are presented as mean ± standard deviation for numerical variables and percentages for categorical variables. χ2 and t tests were used for comparisons between groups, considering p < 0.05 as a significant value.
Results
48 contacts were included (33 women, 69%): mean age 38.8 ± 19 years; distribution by nationality was 27 (56%) Argentinean, 18 (38%) Bolivians and 3 (6%) Peruvians, corresponding to 37 TB cases. Except for one patient, all the individuals had received the BCG vaccine, but 3 of them didn’t have a visible scar. Results of the comparison between groups with positive and negative QTF are shown in Table 1. In two cases (4.2%), the result was indeterminate and so the cases were excluded from the analysis.
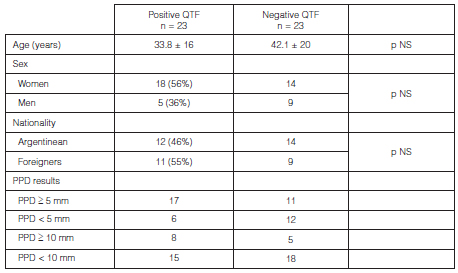
The QTF was positive in 23 (47.9%) cases; there weren’t significant differences between positive and negative cases when considering age (33.8±16 vs. 42.1 ± 20 years), nationality: Argentinean 12 of 26 (46%) vs. foreigners 11 of 20 (55%) and sex: women (18 of 32, 56%) vs. men (5 of 14, 36%).
There were 28 (60.9%) positive cases with PPD-5 and 13 (28.3%) with PPD-10. Comparison between PPD-5 and PPD-10: S = 73.9 vs. 34.8%, E = 52.2 vs. 78.3%, PPV = 60.1 vs. 61.5% and NPV = 66.7 vs. 54.5%, respectively. The coincident results (both positive and negative) between QTF and PPD were
29 (63%) for PPD-5 and 26 (56.5%) for PPD-10. Expressed with the Kappa coefficient, they show weak (0.261) and insignificant (0.130) concordance, respectively.
Discussion
Medical practice in Argentina uses the cutoff point of PPD ≥ 10mm for the diagnosis of LTBI, even though the Argentine consensus proposes the “use of ≥ 5mm in household contacts, in order to sensitize the test giving priority to the detection of individuals with weak tuberculin responses”5. In our work, we compare both PPD cutoff points considering the QTF as reference method, and we observe that within the group of patients under study, the PPD-5 turned out to be more sensitive than the PPD-10 for the diagnosis of LTBI (73.9 vs. 34.8%, respectively) despite a decrease in specificity.
Due to the lack of a gold standard for the diagnosis of LTBI, many studies use the IGRAs as reference tests for their very high specificity. The LTBI is evaluated by studying patients with active TB and non-exposed healthy volunteers by means of the IGRA. The obtained specificity values are 99% (CI 98-100%) for patients who did not receive the BCG and 96% (CI 94-98%) for vaccinated patients6. So, using the QTF as a reference method, the sensitivity values we found are close to the range expressed in similar studies (49 to 68% for PPD-5 and 25 to 50% for PPD-10)3, 7-9 and support the use of PPD-5 as cutoff point in household contacts to reduce the probability of leaving recently infected individuals without chemoprophylaxis. In our study, when using PPD-5, the contacts identified as positive increased from 28.3 to 60.9%.
Though concordance between the QTF and the tuberculin test was low, it was better with PPD-5 than with PPD-10. The low degree of correlation may be related to the fact that the included population is mostly vaccinated, thus increasing positive results with PPD. The BCG is described as the cause of false positive results in the tuberculin test, but, from the clinical point of view, its history shall not be taken into account when interpreting the PPD during the evaluation of household contacts. On the other hand, it has been described that its effect to generate a positive PPD is lost 10 years after its application4.
When comparing the positive and negative QTF groups, we didn’t find significant differences in relation to age, sex or the fact of being a foreigner. The QTF result was indeterminate in two cases (4.2%): a value that was slightly higher than the globally expressed average (3.4%)11.
One limitation to this work, apart from the small sample size of individuals under study, was the fact that a second PPD was not included between 8-12 weeks of the first PPD, to identify conversions in contacts with baseline PPD < 5mm and positive QTF.
A methodological point to emphasize, as regards the reading of the PPD, is that it was performed only by trained personnel (the reference area of our hospital has a TB prevalence of 116/100.000 inhabitants)10. As described in the WHO guides, in countries that do not use IGRA tests as extensively as in our country, the use of the tuberculin test is considered an equivalent method for the diagnosis of LTBI12.
To conclude, we consider that the results obtained in our study support the use of 5 mm as a cutoff point of the PPD for the study of household contacts, due to the higher sensibility of this cutoff point and despite the decrease in specificity. Its concrete use will allow for a greater identification of contacts with recently acquired LTBI, whose treatment is part of the prevention of TB development and one of the pillars to reduce the prevalence of this disease.
Acknowledgement: the vaccination service of the Hospital Parmenio P Piñero and the staff of the Laboratory of Immune Response Study during the infection by Mycobacterium tuberculosis (IQUIBICEN [Institute of Biological Chemistry - School of Exact and Natural Sciences] - UBA [University of Buenos Aires]/CONICET [National Scientific and Technical research Council]).
Conflicts of Interest: VG and NA receive grants from the Secretary of Science and Technique of the University of Buenos Aires (UBACyT, for its acronym in Spanish); NA and NT from the National Agency for Scientific and Technological Promotion (ANPCyT, for its acronym in Spanish).
1. Lewinsohn D, Leonard MK, LoBue PA, et al. Official American Thoracic Society / Infectious Diseases Society of America / Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children. Clinical Infectious Diseases. 2016; 64: 1-33.
2. Kruczak K, Mastalerz L, Sładek K. Interferon-gamma release assays and tuberculin skin testing for diagnosing latent Mycobacterium tuberculosis infection in at-risk groups in Poland. Int J Mycobacteriol. 2016; 5(1): 27-33.
3. Diel R, Loddenkemper R, Niemann S, Meywald-Walter K, Nienhaus A. Negative and positive predictive value of a whole-blood interferon-γ release assay for developing active tuberculosis: an update. Am J Respir Crit Care Med. 2011; 183(1): 88-95.
4. Menzies D. Interpretation of repeated tuberculin tests. Boosting, conversion, and reversion. Am J Respir Crit Care Med. 1999; 159(1): 15-21.
5. Abbate E, Ballester D, Barrera L. Argentine Consensus of Tiberculosis. Rev Argent Med Resp. 2009; 9: 61-99.
6. Pai M, Zwerling A, Menzies D. Systematic review: T-cell-based assays for the diagnosis of latent tuberculosis infection: an update. Ann Intern Med. 2008; 149(3): 177-84.
7. Ferreira TF, Fonseca-Silva P, Miranda A, Mendes-Caldas A. Diagnosis of latent Mycobacterium tuberculosis infection: tuberculin test versus interferon-gamma reléase. Rev Soc Bras Med Trop. 2015; 48(6): 724-730.
8. Reechaipichitkul W, Pimrin W, Bourpoern J, et al. Evaluation of the QuantiFERON®-TB Gold In-Tube assay and tuberculin skin test for the diagnosis of Mycobacterium tuberculosis infection in northeastern Thailand. Asian Pac J Allergy Immunol. 2015; 33: 236-44.
9. Ballaz A, Salinas C, Aguirre U, et al. Analysis of discordance between tuberculin test and QuantiFERON-TB® Gold In-Tube in studies of contacts. Med Clin (Barc). 2013; 140(7): 289-95.
10. 2017 Network for Tuberculosis Care. Government of the City of Buenos Aires, January 25, 2018. RTB/MS/GBA 2018.
11. Cascante JA, Pascal I, Eguía VM, Hueto J. Diagnóstico de la infección tuberculosa. An Sist Sanit Navar. 2007; 30 (Supl. 2): 49-65.
12. Latent tuberculosis infection: updated and consolidated guidelines for programmatic management. Geneva: World Health Organization;2018. Licence: CC BY-NC-SA 3.0 IGO.

| GalerĂa de imĂ¡genes | ||
| Mujer joven con afectaciĂ³n pulmonar bilateral y alteraciĂ³n de la conciencia | ||
Autores: Churin Lisandro |
 |
|